

ARTICULO ORIGINAL
DOI 10.25176/RFMH.v19.n1.1793LEVEL OF KNOWLEDGE AND ATTITUDES ON CHRONIC COMPLICATIONS OF DIABETES MELLITUS 2, HOSPITAL NATIONAL PNP LUIS N. SAENZ, 2016
NIVEL DE CONOCIMIENTOS Y APTITUDES SOBRE COMPLICACIONES CRÓNICAS DE LA DIABETES MELLITUS 2, HOSPITAL NACIONAL PNP. LUIS N. SAENZ, 2016
Aldo Juvenal Calderón-Rivera1
1Hospital Nacional PNP "Luis N. Suárez", Lima-Perú
ABSTRACT
Objective: To determine the relationship between knowledge and aptitude in diabetic patients
regarding the
chronic complications of diabetic mellitus 2 in the Endocrinology Service of PNP National
Hospital Luis N. Suárez
in 2016. Methods: Quantitative, descriptive, transverse and correlational study. 110 diabetic
patients were
surveyed with a questionnaire to assess the knowledge (10 items with a multiple choice
response) and another
one for the skills (modified Lickert type). The knowledge was classified as high, medium and
low level and the
skills as favorable, unfavorable and indifferent according to the Estanones Scale. The
normality of the scores
with the Kolmogorov-Smirnov test and associations with chi-square, p <0.05 and Pearson's
correlation test were determined. Results: The mean age was 49.85 ± 6.97 years, 74.5%
female, 75.5% with disease time between 1-5 years, 67.3% with good adherence to
pharmacological treatment. The level of knowledge was: high 28.2%, medium 49.1% and low
22.7%; And the skills were: favorable 23.6%, unfavorable 58.2% and indifferent 18.2%. There
is no relation between knowledge and skills (p=0.247). Only statistical association was
found between knowledge and pharmacological treatment (p <0.05). Conclusion: Diabetic
patients have an average level of knowledge about their chronic complications and their
abilities were predominantly unfavorable. It is necessary to carry out educational
strategies to improve the knowledge and skills of diabetics.
Key words: Chronic
complications; Diabetic mellitus 2; knowledge; Aptitude; Correlation. (source: MeSH NLM)
RESUMEN
Objetivo: Determinar la relación entre conocimientos y aptitudes en pacientes diabéticos sobre las
complicaciones crónicas de la diabetes mellitus 2 en el Servicio de Endocrinología del Hospital
Nacional PNP
Luis N. Suárez el 2016. Métodos: Estudio cuantitativo, descriptivo, transversal y correlacional. Se
encuestaron
a 110 pacientes diabéticos con un cuestionario para valorar los conocimientos (10 ítems con
respuesta de
selección múltiple) y otro para las aptitudes (tipo Lickert modificado). Los conocimientos se
clasificaron
como nivel alto, medio y bajo y las aptitudes como favorables, desfavorables e indiferentes según
la Escala
de Estanones. Se determinó la normalidad de las puntuaciones con la Prueba de Kolmogorov-Smirnov y
las
asociaciones con chi cuadrado, p<0.05 y prueba de correlación de Pearson. Resultados: La edad media
fue 49.85±6.97 años, 74.5% sexo femenino, 75.5% con tiempo de enfermedad entre 1-5 años, 67.3%
con buena adherencia al tratamiento farmacológico. El nivel de conocimientos fue: alto 28.2%,
medio 49.1% y bajo 22.7%; y las aptitudes fueron: favorables 23.6%, desfavorables 58.2% e
indiferentes 18.2%. No existe relación entre conocimientos y aptitudes (p=0.247). Sólo se
encontró asociación estadística entre conocimiento y tratamiento farmacológico (p<0.05).
Conclusión: Los pacientes diabéticos tienen un nivel de conocimiento medio sobre sus
complicaciones crónicas y sus aptitudes fueron predominantemente desfavorables. Es necesario
realizar estrategias educativas para mejorar los conocimiento y las aptitudes de los
diabéticos.
Palabras clave: Complicaciones crónicas; Diabetes mellitus 2; Conocimientos;
Aptitudes; Correlación. (fuente: DeCS BIREME)
INTRODUCTION
In recent years, diabetes mellitus 2 (DM2) has become a scourge for humanity because of the high morbidity and mortality associated with this disease. Despite technological and therapeutic advances, the metabolic aspects involved have not yet been controlled1,2 to improve the quality of life and prolonging the survival of the patient.
DM2 is a metabolic disease of progressive appearance due to the resistance of the insulin action on its cellular receptors or to the decrease of its pancreatic secretion, which causes hyperglycemia. That will be deposited at the microvascular level and will be responsible for the chronic changes that they will suffer later if the natural history of the disease has not been controlled3,4.
MINSA data are not updated or complete. According to reports from the Office of Statistics and Information from the Ministry of Health in Peru, DM2 affects almost 2 million people and was the 15th cause of death in Peru5. In the study PERUDIAB 2012 carried out in 10 million 25 years old Peruvian adults, Sclén6 found a prevalence of 7% of DM2 and 23% of fasting hyperglycemia considered as prediabetes.
According to Peru Demographic and Family Health Survey (ENDES) 20137 carried out in approximately 7 000 people over 18 years nationally, there is a prevalence of overweight of 33.8% and obesity of 18.3%. Alarming figures, as is known, the DM2 is a consequence of secondary metabolic disorders whose main risk factor is bad eating habits. To this factor can also be added others such as the family history of diabetes, high blood pressure, hypertriglyceridemia, older adults, and women with gestational diabetes2,6,8.
METHODS
An observational, analytical descriptive, cross-sectional, and correlational study was conducted. The study sample was made up of 110 diabetic patients who met the criteria for inclusion and exclusion from the study.
The analysis of the data was carried out in the statistical program SPSS version 22, through a descriptive statistical analysis (percentage distribution of the socio-epidemiological characteristics of the studied diabetic patients and measures of central tendency and standard deviation for age and time of disease). Microsoft Excel was used for the elaboration of the graphs.
To categorize the level of knowledge, we obtained an overall grade of 0 to 10 points. Then the Stanon Scale was made as follows:
• Stanon Scale = Median+-0.75 (standard deviation)
• Higher category (high knowledge level): 4.6+ 0.75(1.6) = 5.8 : >5.8
• Intermediate category (medium level of knowledge): 3.4 - 5.8
• Lower category (low attitude level): 4.6 -0.75(1.6) = 3.4 : <3.4
In the attitudes, each answer was scored according to the range of points: 10-50 points.
The patients were classified according to the score obtained following the Stanon scale:
• Higher category (Favourable): 38.7 + 0.75 (4.0) = 41.7 : > 41.7
• Intermediate category (Unfavourable): 35.7 - 41.7
• Lower category (Indifferent): 38.7 - 0.75 (4.0) = 35.7 : < 35.7
In this way, each subject of study was classified in one of the three categories in both groups, to finally present them in a table with percentage distribution.
The normality of knowledge and attitude level scores was determined by the Kolmogorov-Smirnov test.
The Pearson correlation test was obtained to establish the relationship between knowledge level and skill level on chronic complications of DM2.
The research was carried out according to the principles of bioethics, keeping the data confidential, and maintaining anonymity. The principles of the Declaration of Helsinki were respected and the research ethics committee of the Department of Medicine of the Ricardo Palma University approved the project.
RESULTS
A survey was made of 110 diabetic patients who were treated at the Endocrinology Service of the Luis N. Sáenz National Police Hospital in 2016. The mean age was 49.85±6.97 years, 42.7% were aged 50-59 years, 74.5% were female, 56.4% had higher education, 75.5% had had diabetes mellitus 2 for 1-5 years, insulin drug treatment + oral hypoglycemics 44.5% and 67.3% had good adherence to drug treatment. (Table 1)
Table 1. General characteristics of the diabetic patients surveyed in the endocrinology service of the Hospital of the National Police of Peru "Luis N. Saenz, 2016".
|
Characteristics |
N° % |
|
|
Age groups |
||
|
35-39 |
6 |
5.5 |
|
40-49 |
44 |
40.0 |
|
50-59 |
47 |
42.7 |
|
60-69 |
13 |
11.8 |
|
Sex |
||
|
Male |
28 |
25.5 |
|
Female |
82 |
74.5 |
|
Education level |
||
|
Elementary |
11 |
10.0 |
|
Secondary school |
37 |
33.6 |
|
Higher education |
62 |
56.4 |
|
Time of illness of DM2 |
||
|
1-5 years |
83 |
75.5 |
|
6-10 years |
21 |
19.1 |
|
11-15 years |
4 |
3.6 |
|
16-20 years |
2 |
1.8 |
|
Pharmacological treatment for DM2 |
||
|
Insulin and oral hypoglycemics |
49 |
44.5 |
|
Oral hypoglycemics |
34 |
30.9 |
|
Insulin |
27 |
24.5 |
|
Adherence to pharmacological treatment of DM2 |
||
|
Good |
74 |
67.3 |
|
Bad |
36 |
32.7 |
|
Total |
82 |
100.0 |
Table 2. Kolmogorov-Smirnov test to assess the normal distribution of scores achieved in the level of knowledge and attitudes of diabetic patients.
|
Knowledge |
Attitudes |
||
|
No. |
|
110 |
110 |
|
Parameter |
Medium |
4,62 |
38,67 |
|
normala,b |
Standard deviation |
1,585 |
4,021 |
|
|
Total |
0,134 |
0,160 |
|
More extreme differences |
Positive |
0,134 |
0,059 |
|
|
Negative |
-0,113 |
-0,160 |
|
Kolmogorov-Smirnov Z test |
|
1,400 |
1,675 |
|
Sig. asymptot. (bilateral) |
|
0,040 |
0,007 |
The scores obtained after scoring the answers of diabetic patients in the questionnaires for the level of knowledge and skills presented a normal distribution in the Kolmogorov-Smirnov test. (Table 2)
Figure 1. Level of knowledge of diabetic patients about chronic complications of diabetes mellitus 2. Service of Endocrinology of the Hospital of the National Police of Peru Luis N. Saenz, 2016

Se encontró que el 49.1% tenía nivel medio en conocimientos sobre complicaciones de la DM2, 28.2% nivel alto y 22.7% nivel bajo. (Figura 1)
Figure 2. Attitude of diabetic patients on chronic complications of diabetes mellitus 2. Endocrinology Service of the Hospital de la Policía Nacional del Perú Luis N. Sáenz, 2016

It was found that 58.2% of the diabetics surveyed had unfavorable attitudes, 23.6% favorable attitudes, and 18.2% unimportant attitudes. (Figure 2)
Table 3. Kolmogorov-Smirnov test to assess the normal distribution of scores achieved in the level of knowledge and attitudes of diabetic patients.
|
LEVEL OF KNOWLEDGE |
ATTITUDES |
||||||
|
INDIFFERENT |
UNFAVORABLE | FAVORABLE | P | ||||
| N° | % | N° | % | N° | % | ||
|
Low |
8 |
40.0 |
14 |
21.9 |
3 |
11.5 |
0.247 |
|
Medium |
7 |
35.0 |
32 |
50.0 |
15 |
57.7 |
|
|
High |
5 |
25.0 |
18 |
28.1 |
8 |
30.8 |
|
|
Total |
25 |
100.0 |
54 |
100.0 |
31 |
100.0 |
|
Diabetics patients with a medium-low level of knowledge (50% and 21.9%) have unfavorable attitudes, but among those with favorable attitudes, few had a low level of knowledge (11.5%). There is no statistical association between attitudes and knowledge level (p>0.05) (Table No. 3).
Figure 3. Attitudes and level of knowledge of diabetic patients Endocrinology Service of the Hospital of the National Police of Peru Luis N. Saenz, 2016
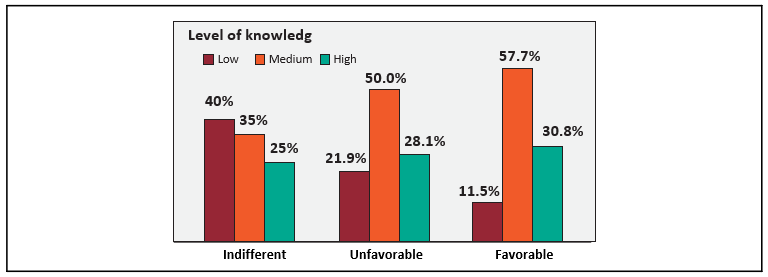
The low level of knowledge predominates in diabetic patients with indifferent and unfavorable attitudes (Figure 3).
Table 4. Association between the level of knowledge of chronic complications of DM2 and the characteristics of diabetic patients Endocrinology Service of the Peruvian National Police Hospital "Luis N. Sáenz, 2016".
|
LEVEL OF KNOWLEDGE |
P |
||||||
| LOW | MEDIUM | HIGH | |||||
| N° | % | N° | % | N° | % | ||
|
Age group |
|||||||
|
35-39 years |
1 |
4.0 |
4 |
7.4 |
1 |
3.2 |
|
|
40-49 years |
7 |
28.0 |
21 |
38.9 |
16 |
51.6 |
0.314 |
|
50-59 years |
11 |
44.0 |
24 |
44.4 |
12 |
38.7 |
|
|
60-69 years |
6 |
24.0 |
5 |
9.3 |
2 |
6.5 |
|
|
Sex |
|||||||
|
Male |
5 |
20.0 |
11 |
20.4 |
12 |
38.7 |
0.135 |
|
Female |
20 |
80.0 |
43 |
79.6 |
19 |
61.3 |
|
|
Education level |
|||||||
|
Elementary |
4 |
16.0 |
6 |
11.1 |
1 |
3.2 |
0.577 |
|
Secondary |
7 |
28.0 |
18 |
33.3 |
12 |
38.7 |
|
|
Higher education |
14 |
56.0 |
30 |
55.6 |
18 |
58.1 |
|
|
Time of illness |
|||||||
|
1-5 years |
15 |
60.0 |
46 |
85.2 |
22 |
71.0 |
0.066 |
|
6-10 years |
7 |
28.0 |
7 |
13.0 |
7 |
22.6 |
|
|
11-15 years |
1 |
4.0 |
1 |
1.9 |
2 |
6.5 |
|
|
16-20 years |
2 |
8.0 |
0 |
0.0 |
0 |
0.0 |
|
|
Pharmacological treatment |
|||||||
|
Insulin and oral hypoglycemics |
11 |
44.0 |
17 |
31.5 |
7 |
22.6 |
0.024 |
|
Oral hypoglycemics |
7 |
28.0 |
20 |
37.0 |
3 |
9.7 |
|
|
Insulin |
7 |
28.0 |
17 |
31.5 |
21 |
67.7 |
|
|
Adherence to pharmacological treatment of DM2 |
|||||||
|
Good |
17 |
68.0 |
33 |
61.1 |
24 |
77.4 |
0.303 |
|
Poor |
8 |
32.0 |
21 |
38.9 |
7 |
22.6 |
|
|
Total |
25 |
100.0 |
54 |
100.0 |
31 |
100.0 |
|
By stratifying the level of knowledge according to the characteristics of the diabetic patients, it was found that those with a low level of knowledge were 50-59 years old (44%), female (80%), with higher-level education (56%), a time of illness of 1-5 years (60%), they received insulin + oral hypoglycemics as drug treatment (44%), and poor drug adherence (35%). Diabetics patients with the highest level of knowledge were 40-49 years old (51.6%), female (61.3%), with secondary education (58.1%), 1-5 years of DM2 disease (71%), insulin treatment (67.7%), and poor drug adherence (22.6%). A statistically significant association was found only with pharmacological treatment of DM2 (p<0.05).(Table4)
Table 5. Association between unfavorable attitudes level regarding chronic complications of DM2 and characteristics of diabetic patients. Endocrinology Service of the Peruvian National Police Hospital "Luis N. Sáenz, 2016".
|
LEVEL OF KNOWLEDGE |
P |
||||||
| LOW | MEDIUM | HIGH | |||||
| N° | % | N° | % | N° | % | ||
|
Age group |
|||||||
|
35-39 years |
0 |
0.0 |
5 |
7.8 |
1 |
3.8 |
0.072 |
|
40-49 years |
7 |
35.0 |
28 |
43.8 |
9 |
34.6 |
|
|
50-59 years |
7 |
35.0 |
25 |
39.1 |
15 |
57.7 |
|
|
60-69 years |
6 |
30.0 |
6 |
9.4 |
1 |
3.8 |
|
|
Sex |
|||||||
|
Male |
2 |
10.0 |
19 |
29.7 |
7 |
26.9 |
0.207 |
|
Female |
18 |
90.0 |
45 |
70.3 |
19 |
73.1 |
|
|
Education level |
|||||||
|
Elementary |
4 |
20.0 |
6 |
9.4 |
1 |
3.8 |
0.280 |
|
Secondary |
5 |
25.0 |
20 |
31.3 |
12 |
46.2 |
|
|
Higher education |
11 |
55.0 |
38 |
59.4 |
13 |
50.0 |
|
|
Time of illness |
|||||||
|
1-5 years |
12 |
60.0 |
52 |
81.3 |
19 |
73.1 |
0.055 |
|
6-10 years |
4 |
20.0 |
11 |
17.2 |
6 |
23.1 |
|
|
11-15 years |
3 |
15.0 |
0 |
0.0 |
1 |
3.8 |
|
|
16-20 years |
1 |
5.0 |
1 |
1.6 |
0 |
0.0 |
|
|
Pharmacological treatment for DM2 |
|||||||
|
Oral hypoglycemics |
11 |
55.0 |
29 |
45.3 |
9 |
34.6 |
0.727 |
|
Hipoglicemiantes orales |
5 |
25.0 |
19 |
29.7 |
10 |
38.5 |
|
|
Insulin |
4 |
20.0 |
16 |
25.0 |
7 |
26.9 |
|
|
Adherence to pharmacological treatment of DM2 |
|||||||
|
Good |
13 |
65.0 |
43 |
67.2 |
18 |
69.2 |
0.955 |
|
Poor |
7 |
35.0 |
21 |
32.8 |
8 |
30.8 |
|
|
Total |
20 |
100.0 |
64 |
100.0 |
26 |
100.0 |
|
By stratifying the attitude level according to the characteristics of the diabetic patients, it was found that those with unfavorable attitudes were 40-49 years old (43.8%), female (70.3%), with higher education (59.4%), a time of illness of 1-5 years (81.3%), they received pharmacological treatment insulin + oral hypoglycemics (45.3%) and poor pharmacological adherence (32.8%). Diabetics with a favorable attitude were 50-59 years old (43.8%), female (73.1%), with higher education (50%), a time of disease of 1-5 years (73.1%), and as the pharmacological treatment they received oral hypoglycemics (38.5%) and poor pharmacological adherence (30.8%). No statistically significant association was found between attitude level and any characteristic of diabetic patients. (Table 5)
DISCUSSION
In the study, 110 patients were surveyed. The average age was 49.85±6.97 years, with a predominance of 50-59 years (42.7%) similar to the study by Morales12 in Nicaragua, Aguilar, and Espinoza16 in Bolivia (67% and 80% were >51 years old, respectively). However, the average ages were higher than that of the patients in the Loayza Hospital evaluated by Yance (average age 44.5+-16.6 years) and lower than the Mendizabal series18 in the Carrión del Callao National Hospital (average age 55.6 years) and the Untiveros study21 in the Dos de Mayo National Hospital (64.56 ± 11.61 years). The female sex predominated (74.5%) as in Morales12 (84%), Aguilar y Espinoza16 (71%), Yance14 (71%), Mendizabal18 (70.8%) and Untiveros21 (56.4%) study. Likewise, it was found that the diabetics in the series were mostly highly educated (56.4%) similar to the Yance study (53%) but contrary to the Mendizabal18 study in which the lower educated predominated.
Regarding the time of DM2 disease, 75.5% of our diabetic patient surveyed was 1-5 years old, although the series of Yance14 and Morales12 showed a predominance of this same length of time, but with lower percentages (54% and 56% respectively). The literature confirms that there is an epidemiological increase in DM2 and the age of appearance of the disease is in increasingly younger and economically active populations24,26,32.
The most used drug treatment was the combination of insulin + oral hypoglycemics (44.5%). Although in other national studies the use of oral hypoglycemics was predominant as reported by Untiveros21 (68.1% oral hypoglycemics vs. 11.7% insulin).
67.3% of the patients studied had good adherence to drug treatment and 32.7% had poor adherence. These characteristics are similar to Molina study19 who found good adherence of 68.9% in patients of the Hospital Nacional Dos de Mayo. This data is within the range described by the medical literature. In other words, between 20 and 40% of diabetic patients have poor adherence to drug treatment, in which insulin therapy is used more.
Approximately half of the respondents knew about chronic complications of DM2 at a medium or regular level. Only 28.2% had a high level of knowledge. These results are similar to Yance study14 in diabetics from Loayza Hospital, where the average level of knowledge was 64% and presented a lower percentage of the bad level than our study (14% vs. 22.7% respectively). This is contrary to what we expected to find since these patients are within a diabetes program. They have not only medical consultation but also health promotion and prevention activities. In other words, a greater number of diabetics should have a high level of knowledge. Although the study does not aim to identify the factors that are involved, it can be intuited that there is shared responsibility between medical personnel and the patient-family28.
The research allows us to appreciate some differences between diabetics with a high and low level of knowledge of the chronic complications of DM2. Thus, when looking at age, those over 50 tend to have a low level, while those under 50 have a higher level of knowledge. In terms of gender, women predominate as a percentage of men at all levels of knowledge, but it can be seen that men have more percentage in the high level of knowledge than women. A significant statistical association was demonstrated between the level of knowledge and pharmacological treatment. Thus, those with a high level of knowledge were mostly patients using insulin while the low level corresponded to a higher proportion of patients with the combination of insulin + oral hypoglycemics (p<0.05). It is evident that the higher the level of knowledge, the greater the proportion of patients with good adherence to drug treatment, although this did not have statistical significance for the study (p>0.05). No major difference is observed in the level of knowledge with the degree of education and time of illness of the diabetic patient.
The research showed a higher proportion of diabetic patients with unfavorable attitudes (58.2%) than favorable attitudes (23.6%). A finding similar to that reported by Yance14 who in his study found unfavorable attitudes in 53% and favorable attitudes in 37%. These data are contrary to expectations if we take into account the study byTello13 which found a higher percentage of favorable attitudes in healthy workers (57%), those who do not receive more information about the diabetic disease, but who have a better attitude toward self-care. Therefore, intervention strategies should not only include knowledge, but also the adoption of attitudinal changes that allow the achievement of metabolic objectives and the practice of promotional preventive measures to prevent or slow the progression of chronic complications of DM225-28-32.
CONCLUSION
The research found that diabetic patients have not yet reached the objectives of the Diabetes Program of the Endocrinology Service of the Luis N. Saenz National Police Hospital, regarding the acquisition of knowledge and achievement of changes in the attitude toward self-care as a strategy to prevent chronic complications of diabetes mellitus 2. They have mostly an unfavorable level of knowledge and attitudes for chronic complications of diabetes mellitus 2.
The research did not find a relationship between the level of knowledge and level of attitudes in the diabetic patients surveyed but there is evidence of a statistically significant association between level of knowledge and drug treatment of diabetes mellitus 2.
RECOMENDATIONS
The authorities of the Ministry of Health and the Hospital of the National Police of Peru Luis N. Saenz should redesign the educational strategies of the Diabetes Program to increase the level of knowledge about chronic complications of DM2, as well as to modify behaviors and bad habits in diabetic patients to allow them to integrate into their health care.
Despite the fact that low adherence to drug treatment is similar to that described in the literature. It is recommended to carry out prospective studies, of cause-effect design to identify the causes for which it has not been possible to improve the intellectual and attitudinal capacities of the patients or studies of an educational intervention that allow raising the knowledge of the diabetics about their disease. These studies will value the impact of the actions taken, so the changes will be able to be made to introduce improvements in quality in professional attention.
Authorship contributions: The author carried out the research, information gathering, writing, and final approval of the original article.
Financing: Self-financed.
Conflict of interest: The author declares no conflict of interest in the publication of this article..
Received: August 21, 2018
Approved: December 19, 2018
Correspondence: Aldo Juvenal Calderon Rivera
Address: Psje San Francisco 135-Los Laureles Chorrillos.
Telephone: +51991887134
Email: ajcalderonrivera@gmail.com
BIBLIOGRAPHICAL REFERENCES
1.Braden B, Enghofer M, Schaub M, et al. Long-term cisapride treatment improves diabetic gastroparesis but not glycaemic control. Aliment Pharmacol Ther 2002; 16: 1341-6.
2. Dandamudi S, Slusser J, et al. The prevalence of diabetic cardiomyopathy: a population-based study in Olmsted County, Minnesota. J Card Fail 2014; 20(5): 304-306
3. Del Favero G, Caroli A, Meggiato T, et al. Natural history of gallstones in non-insulin-dependent diabetes mellitus. A prospective 5-year follow-up. Dig Dis Sci 1994; 39(8): 1704-7.
4. Espinás J, Salla RM, Bellvehi M, et al. Reevaluación del programa de diabetes mellitus tipo 2. Propuesta de indicadores de calidad. Aten Primaria 1993; 11: 123-126.
5. Fernández J, Iza A, Lasa I, et al. Evaluación de la población diabética tipo II atendida en un equipo de atención primaria. Aten Primaria 1996; 17: 432-438.
6. Fernández Suárez F, Trueba A, Ferrús JA. Influencia de un programa de atención al diabético sobre su control. Aten Primaria 1995; 15: 341-348.
7. Figuerola D, Recasens C, Castell C, Lloveras G. La asistencia al diabético en Cataluña. Estudio en una muestra de población. Med Clin 1992; 99: 90- 95.
8. Kalra S, Unnikrishnan AG, Baruah MP. Diabetes therapy by the ear. Indian J Endocrinol Metab 2013; 17(3): 596-598
9. Koskinen P, Manttari M, Manninen V, Huttunen JK, Heinonen OP, Frick MH. Incidencia de cardiopatía coronaria en pacientes con DMNID en el estudio cardiológico de Helsinki. Diabetes Care 1992; 15: 820-825
10. Ortega M.C. Tratamiento de la neuropatía autonómica diabética. Formación Médica Continuada en Atención Primaria 2005; 12(9): 618-30.
11. Stumvoll M, Goldstein BJ, van Haeften TW. Type 2 diabetes: principles of pathogenesis and therapy. Lancet 2005; 365: 1333-46.
