Dear Editor
Gallbladder cancer is one of the most common pathologies of the digestive tract. It is more frequent in women than in men predominantly in the sixth and seventh decades of life. In white populations, it is a type of neoplasm that ranks fifth worldwide1.
Usually, gallbladder cancer causes no signs or symptoms until later in the course of the disease, when the tumor is large or has spread. The vesicular pathology has been increasing over the years since there is no proper prevention. Many of the risk factors, such as age, sex and others that vary like diabetic women, smoking, obesity with the presence of stones2.
Chile has the highest incidence of vesicular cancer, between men and women. According to the study of Eslick published in 2010, the rate of the registry of the city of Valdivia is 12.3 and 27.3 in men and women per 100,000 inhabitants, placing it with the highest incidence in the world - data from the Ministry of Health of Chile3.
In 2010-2012 according to the INEN - MINSA (National Institute of Neoplastic Diseases - Ministry of Health), in metropolitan Lima, there were 1284 cases of gallbladder cancer. The population most affected by this pathology were adults older than 75 years old. By age group and sex, it was predominant in women, increasing from 3.2% in women from 55 to 74 years to 3.5% in 75 years to more4.
The onset of symptoms is insidious and simulates cholecystitis; often the diagnosis is established during gallbladder surgery from other cause. About 80-90% of people with gallbladder cancer have cholelithiasis. It is believed that, due to its ability to produce chronic irritation of the vesicular mucosa, cholelithiasis participates in the development of cancer. This cancer is unresectable at the time of diagnosis and the average survival at five years has been 1% for many years. Gallbladder cancer is the most frequent malignant tumor of the bile ducts1.
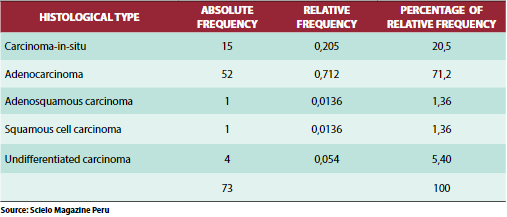
In an analytical observational study, cross-sectional and retrospective that was performed in the surgical service of the Hospital Regional Honorio Delgado (HRHD) of Arequipa during the period from January 2008 to June 2010, the population consisted of all patients who attended the service of surgery that underwent surgery, the operative piece was sent to the pathology department for processing. The criterion was to have a result (report) of pathology.There was evidence that 73 patients had a diagnosis of gallbladder cancer. The most common histological type was adenocarcinoma with 71.2% (52 cases), followed by in-situ carcinoma with 20.5% (15 cases), both histological types representing 91.7%. Undifferentiated carcinoma was present with 4 cases5.
Table 1.Case frequency of patients with gallbladder cancer according to histological type during the period of 2005-2010 in the Hospital Honorio Delgado of Arequipa.
According to the studies, the majority of cancers are adenocarcinomas that grow from the gallbladder mucosa; therefore, it is known that chronic inflammation can be the trigger for the progression of dysplasia to carcinoma in susceptible patients since most of these factors are related to inflammation. Those more significant than 30 mm have a higher risk by 10 times more to develop vesicular cancer. The size, weight, quantity, and density of the stones are increased in this neoplasm.
The advent of the laparoscope, compared to historical controls, makes this disease diagnosed more often incidentally and at an earlier stage. However, when the symptoms of jaundice and pain are present, the prognosis remains dismal
6.
With the wide availability of ultrasonography, cholecystectomy has become the most frequent surgical procedure in the world. As a result of this, an increase in incidental vesicular cancer is expected. Incidental carcinoma of the gallbladder is usually diagnosed in the early stages and carries a better prognosis than non-incidental cancers
7.
Patients with porcelain gallbladder have the possibility of developing cancer above 25%. Any patient older than 50 years with a solitary polyp in the gallbladder greater than 1 cm should undergo laparoscopic cholecystectomy with a freeze biopsy of the polyp. Patients with less than three polyps regardless of size should be considered for laparoscopic cholecystectomy if the morbidity of resection is minimal. Patients that are high risk for general anesthesia should be observed with ultrasound every 6 months. Patients with more than three polyps are likely to have pseudotumor and can be seen without surgery unless they have symptoms of biliary colic. Patients with suspicious findings on an ultrasound examination, with a porcelain vesicle, and with large solitary polyps should be managed with open cholecystectomy and biopsy of the suspicious lesion to minimize the seeding of tumor cells
8.
 Figure 1.Radiographic image of patient diagnosed with gallbladder cancer. Cholecystectomy with diagnosis of gallbladder cancer
Figure 1.Radiographic image of patient diagnosed with gallbladder cancer. Cholecystectomy with diagnosis of gallbladder cancer
 Figure 2.Surgical piece extracted
Figure 2.Surgical piece extracted
 Figure 3.Surgical piece extracted.
Figure 3.Surgical piece extracted.
The present communication seeks to identify the clinical and epidemiological factors related to vesicular cancer; in addition, it identifies which type according to the pathological anatomy is the most prevalent; as well as taking into account the most frequent sociodemographic profile in overweight or obese women
Correspondence:Kelly Regina Huacachi Trejo.
Address::Jr. Los Laureles 352. Dpto. 402. Santiago de Surco.
Telephone:+51 999115611.
E-mail: kelita_bht¬@hotmail.com
BIBLIOGRAPHIC REFERENCES
1. Pellisé M, Castells A. Tumores de la Vesícula y Vías Biliares. Servicio de
Gastroenterología. Hospital Clínic de Barcelona. 2012; 5(47): 689 – 697.
3. Uribe M, Heine C, Brito F, Bravo D. Actualización en cáncer de vesícula biliar
[REV. MED. CLIN. CONDES - 2013; 24(4) 638-643]
4. Jefatura Institucional, Dirección de Control del Cáncer, Departamento
de Epidemiología y Estadística. Registro de Cáncer de Lima Metropolitana
Incidencia y Mortalidad 2010 – 2012. Perú: INEN y Departamento de
Epidemiología y Estadística del Cáncer. 2016; 5.
5. Gamarra R, Coapaza Y, Salazar F, Ojeda Y. Cáncer de vesícula biliar según
tipo histológico y clasificación TNM en Arequipa, Perú. Acta méd. peruana
v.29 n.1 Lima ene./mar. 2012
6. Wernberg, J, Lucarelli D. Gallbladder Cancer. Elsevier Inc. Washington
2014; 94: 343-360
7. Cavallaro A, Piccolo G, Di Vita M, Zanghi, Cardí F, Di Mattia P, BarberaG, et
al. Managing the incidentally detected gallbladder cancer: Algorithms and
controversies. International Journal of Surgery. 2014; 12: S108 – S119.
8. Ríos P, Aguilar L, Rios P. Cancer de vesicula biliar- estrategia quirúrgica: a
propósito de un caso incidental re-resecado en el hospital Rebagliati. Rev.
gastroenterol. Perú v.29 n.4 Lima oct./dic. 2009




