ORIGINAL ARTICLE
JOURNAL OF THE FACULTY OF HUMAN MEDICINE 2020 - Universidad Ricardo PalmaDOI 10.25176/RFMH.v20i2.2881
PREVALENCE AND FACTORS ASSOCIATED WITH DEPRESSIVE SYMPTOMATOLOGY IN OLDER ADULTS OF THE “MICAELA BASTIDAS” HEALTH CENTER, LIMA-PERU
PREVALENCIA Y FACTORES ASOCIADOS A SINTOMATOLOGÍA DEPRESIVA EN ADULTOS MAYORES DEL CENTRO DE SALUD “MICAELA BASTIDAS” LIMA-PERÚ
Christian Ponce-Torres1,
Luigui Viteri-Condori1,
Pablo Ramos-Martínez1,
Wendy Nieto-Gutiérrez1,
Jesus Cueva-Velazco 1
1Facultad de Medicina Humana de la Universidad de San Martin de Porres, Lima - Perú.
ABSTRACT
Objective: To evaluate the factors associated with depressive symptomatology in older adults attending to “Micaela Bastidas” health center from Lima, Peru. Methods: Cross-sectional analytical study in adults over 60 in a marginal urban area from Lima. We evaluated the dependent variable using the geriatric depression scale of 15 items. We considered the presence of depressive symptomatology with a score ≥ 6. We calculated the factors associated with depressive symptomatology using raw and adjusted prevalence ratios with 95% confidence intervals (95% CI) using poisson regressions with robust variance. Results: Of the 142 older adults (age 70.4 ± 8.14 years old), the prevalence of the presence of depressive symptomatology was 55.6% (women: 39.6% and men: 53.4%). The lack of schooling (RPa: 1.40, 95% CI: 1.04 - 1.88) and not working (RPa: 1.50, 95% CI: 1.09 - 2.05) were risk factors that increased the prevalence of depressive symptomatology. Conclusion: The prevalence of presence of depressive symptomatology in older adults from a marginal urban area of Peru was high. Older adults who did not complete their schooling and did not work were more likely to develop depressive symptomatology.
Key words:Depression, Old people, preventive health services (source: MeSH NLM).
RESUMEN
Objetivo: Evaluar los factores asociados a la sintomatología depresiva en adultos mayores residentes del centro de salud asistentes al centro de salud “Micaela Bastidas” de Lima-Perú.
Métodos: Estudio transversal analítico en adultos mayores de 60 años residentes de una zona urbano marginal de Lima. Se evaluó la variable dependiente usando la escala de depresión geriátrica de 15 ítems, se consideró la presencia de sintomatología depresiva con un puntaje ≥ 6. Los factores asociados a la sintomatología depresiva, se calcularon usando razones de prevalencia crudas y ajustadas con intervalos de confianza al 95% (IC 95%) mediante regresiones de poisson con varianza robusta.
Resultados: De los 142 adultos mayores (edad 70,4 ± 8,14 años), la prevalencia de la presencia de sintomatología depresiva fue 55,6% (mujeres: 39,6% y hombres; 53,4%). El no tener escolaridad (RPa: 1,40; IC 95%: 1,04 – 1,88) y no estar trabajando (RPa: 1,50; IC 95%: 1,09 – 2,05) fueron factores asociados que aumentaban la prevalencia de sintomatología depresiva.
Conclusión: La prevalencia de presencia de sintomatología depresiva en adultos mayores de una zona urbano marginal de Perú fue alta. Los adultos mayores que no completaron su escolaridad y no trabajaban presentaron más probabilidades de presentar sintomatología depresiva.
Palabras clave: Depresión; Anciano; Servicios preventivos de salud (fuente: DeCS BIREME).
Depression is one of the most important neuropsychiatric disorders in elderly, and one of the causes of disability that diminishes physical, cognitive and social functionality, thus, it affects quality of life and wellbeing(1).
By the year 2017, the World Health Organization (WHO) estimated a prevalence of depression of 7% in elderly over 60(2). Nevertheless, studies have reported variable figures regarding elderly with depression which differs according to the context in terms of assistance in patients in hospitalization: 32.8% in Chengdu, China(3); 44% in East Anglia, United Kingdom(4); 47% in Belo Horizonte, Brazil(5). In outpatients: 22% in Bikaner, India(6); 29.9% in Izmir, Turkey(7). In primary care centers: 39.6% in Ethekwini, South Africa(8); 45.3% in Kavre, Nepal(9); 47.2% in Beirut, Lebanon(10). In elderly from the community: 27.8% in Sri Lanka, Singapore(11); 29.5% in Antioquia, Colombia(12); 36% in Bangalore, India(13); 52.6% in Vitoria da Conquista, Brazil(14).
Concerning factors associated with geriatric depression, we have reported in literature with most frequency the fact of being a woman(8,15,16), lack of schooling(15,17), cognitive impairment(16,17), living single(8,16), suffer from health problems(18,19), previous hospitalizations(19), lack of social support(19,20), low socioeconomic status(16), not working(21) ,etc.
There are scales that serve as screening instruments to evaluate depressive symptomatology in geriatric population, including, Scale Geriatric Depression (GDS) created by Yesavage et al, in year 1983. It originally consists of 30 questions with dichotomous answers (yes or no)(22), This scale is frequently used in epidemiological studies of depression in elderly. In our research of Peruvian studies published about this topic that had used GDS, in his short version of 15 questions, we have mostly reported high numbers of depression. 51.6% (with a score of five or more) in an AA.HH. (short for Asentamiento Humano. Human Settlement in English) from La Molina district, Lima(23); 8.4% (with a score of six or more) in the community from San Martín de Porres district, Lima(24); Also, 48.2% (with a score of six or more) in the community from Breña district, Lima(25); and 69.4% in the community from Masma Chicce, Junín(26); 64.9% in a national hospital from Ica, Ica(27) In these two last studies, there is not a description about the cut-off point of GDS-15.
There are few published research about depression in elderly from marginal urban communities, taking into account their poverty situation and poor access to mental health services. This may complicate planning preventive strategies that improve early detection of depressive symptoms and maintain functionality of this age group.
For this reason, the objective of this study is to determine factors associated with depressive symptomatology in elderly living in a marginal urban area, the “AA.HH. Micaela Bastidas I” located in Ate Vitarte district in Lima, Peru.
METHODS
Design and place of study
We carried out an observational, analytic and cross-sectional study in elderly age 60 or over from AA.HH. Micaela Bastidas I in Lima, from April 2014 to July 2014.
The “AA.HH. Micaela Bastidas I” is a marginal urban area, founded on year 1985, located in Ate Vitarte district in Eastern Lima. Its inhabitants have low socioeconomic status. This town counts with a primary care center Micaela Bastidas level I-3 from MicroRed Ate II of Health Ministry.
Population and Sample
The participants were 200 60-year-old elderly in year 2014 who attended to Micaela Bastidas health center. We conducted a survey to every elderly. Among the eligibility criteria, we included elderly who were attended at “Micaela Bastidas” health center during study period and who had accepted participating through a signed informed consent. We did not include those elderly with some kind of cognitive impairment who were previously diagnosed by a doctor; information provided by health center as we can observe in Figure 1elderly responded, after a quality control we deleted four questionnaires that were incomplete. Final sample was of 142 participants, obtaining an answer from 71% of total of elderly.
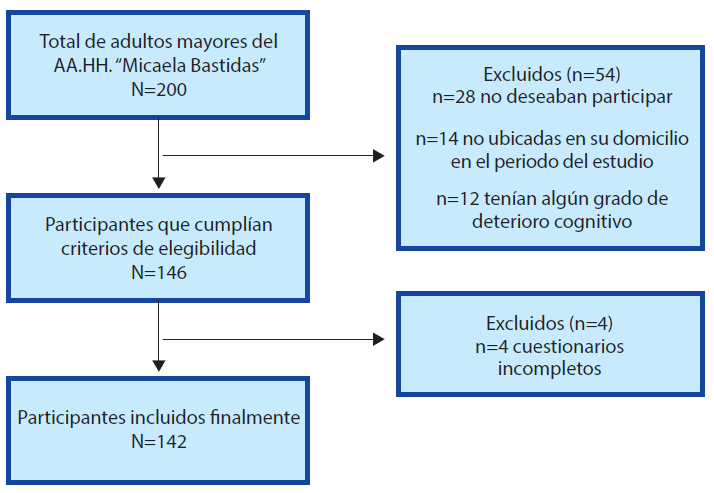
Figure 1. Inclusion diagram of participant in the study
Procedures
The authors of the study were in charge of data collection through interviews with every elderly. We requested permission to health center “Micaela Bastidas” to interview those elderly who went to the establishment for a medical appointment. In addition, each interviewer visited three times a week the homes of “AA.HH. Micaela Bastidas” based on a street and block plan of the area. In every home, we asked if there was an elderly over 60 living inside. Participation in the study was voluntary; we informed previously about the objectives of the study and informed consent to the participants.
Variables
Dependent variable of interest was depressive symptomatology in elderly. For this purpose, we applied Yesavage et al. GDS-15 scale. We have approved and applied this scale widely with worldwide multiple population of elderly(22). In this study, we applied the version translated to Spanish of Questionnaire GDS-15. It contains 15 questions in total. Each question is worth a point. Answers are dichotomous: yes or no. Of 15 points, a score over or equal to six points suggests presence of depressive symptoms(28).
In terms of independent variables, we selected them from similar studies: sex; age (in tertiles); marital status was categorized into those with partner (those who were married or cohabiting partners) and without partner (single, widowers or divorced). Also, level of education into without schooling (without studies or incomplete primary) and with schooling (complete primary, secondary or higher education); origin (Lima or other cities in Peru); health problem told by the participant (yes or no); and belonging to an elderly club (yes or no).
Data analysis
We exported Database in Microsoft Excel 2010 to STATA software version 13. In the descriptive analysis, we used absolute and relative frequencies. For evaluating factors associated with depressive symptoms, we made use of poisson regressions with robust variance and we calculated prevalence ratios (PR) and its confidence interval to 95%, considering statistical significance as p<0.05. For adjusted models. We included variables: sex, age, level of education, marital status, origin, health problems and elderly club.
Ethical aspects
In this investigation, we followed ethical principles of Helsinki Declaration. Participation in the study was always voluntary. We maintained data confidentiality and participants were not exposed to any other type of risk for their contribution. We exposed previously a written and oral informed consent to participants. At the end, we handed the results to health center Micaela Bastidas.
RESULTS
In total, 142 elderly accepted to participate in the study: 67.6% were women, average age and standard deviation was 70.4±8.14. 43.7% were married. Most of the participant (85.9%) came from other cities, 69.0% expressed having a health problem and 71.8% did not belong to any elderly club. Regarding GDS-15 score, 44.4% obtained from 0 to 5 points (without depressive symptoms); 43.7%, from 6 to 10 points (risk of depressive symptomatology); and 12.0%, from 11 to 15 points (established depressive symptomatology) (Table 1).
Table 1. Sociodemographic data and GDS-15 scale in study population (n=142)
| Variables | N (%) |
| Sex | |
| Female | 96 (67,6) |
| Male | 46 (32,4) |
| Marital status | |
| Married | 62 (43,7) |
| Partner | 10 (7,0) |
| Divorced | 13 (9,2) |
| Single | 2 (1,4) |
| Widower/Widow | 55 (38,7) |
| Level of education | |
| Illiterate | 28 (19,7) |
| Incomplete Primary | 38 (26,8) |
| Complete Primary | 28 (19,7) |
| Incomplete Secondary | 14 (9,9) |
| Complete Secondary | 29 (20,4) |
| Higher Education | 5 (3,5) |
| Origin | |
| Lima | 20 (14,1) |
| Province | 122 (85,9) |
| Health problems | |
| No | 44 (31,0) |
| Yes | 98 (69,0) |
| Belongs to an elderly club | |
| No | 102 (71,8) |
| Yes | 40 (28,2) |
| Job situation | |
| Not working | 74 (52,1) |
| Working | 68 (47,9) |
| GDS-15 score | |
| Normal | 63 (44,4) |
| Risk of depressive symptomatology | 62 (43,7) |
| Established depressive symptomatology | 17 (12,0) |
Regarding factors associated with having depressive symptoms (GDS-15 with a score of ≥6 points), we found in adjusted analysis the following variables: lack of schooling (RP=1.40; CI95%:1.04 - 1.88) and not working (RP: 1.50; CI95%:1.09 - 2.05). We did not discover significant association with sex, age, partner, origin, health problems and belonging to an elderly club (Table 2).
Table 2. Factors associated to depression in elderly
| Risk of depressive symptomatology | ||||
| Variables |
Without depressive symptomatology N (%) 63 (44,4%) |
With depressive symptomatology N(%) 79 (55,6%) |
Raw RPc (IC95%) |
Adjusted RPa (IC95%) |
| Sex | ||||
| Female | 38 (39,6) | 58 (60,4) | Ref | Ref |
| Male | 25 (54,3) | 21 (45,7) | 0,76 (0,53 - 1,08) | 0,87 (0,63 - 1,21) |
| Age | ||||
| Between 60 and 68 years old | 34 (47,9) | 37 (52,1) | Ref | Ref |
| Between 69 and 90 years old | 29 (40,8) | 42 (59,2) | 1,14 (0,84 - 1,53) | 0,99 (0,73 - 1,33) |
| Marital status* | ||||
| With partner | 36 (50,0) | 36 (50,0) | Ref | Ref |
| Without partner | 27 (38,6) | 43 (61,4) | 1,23 (0,91 - 1,65) | 1,23 (0,92 - 1,64) |
| Level of education | ||||
| Schooled | 42 (55,3) | 34 (44,7) | Ref | Ref |
| Unschooled | 21 (31,8) | 45 (68,2) | 1,52 (1,13 - 2,06) | 1,40 (1,04 - 1,88) |
| Origin | ||||
| Lima | 12 (60,0) | 8 (40,0) | Ref | Ref |
| Province | 51 (41,8) | 71 (58,2) | 1,46 (0,84 - 2,54) | 1,35 (0,85 - 2,16) |
| Health problems | ||||
| Does not present | 24 (54,5) | 20 (45,5) | Ref | Ref |
| Does present | 39 (39,8) | 59 (60,2) | 1,32 (0,92 - 1,90) | 1,18 (0,82 - 1,69) |
| Belongs to an elderly club | ||||
| Yes | 17 (42,5) | 23 (57,5) | Ref | Ref |
| No | 46 (45,1) | 56 (54,9) | 0,95 (0,69 - 1,32) | 1,10 (0,79 - 1,52) |
| Job situation | ||||
| Does work | 39 (57,4) | 29 (42,6) | Ref | Ref |
| Does not work/td> | 24 (32,4) | 50 (67,6) | 1,58 (1,15 - 2,18) | 1,50 (1,09 - 2,05) |
DISCUSSION
Percentages of depression
Of the total (142 elderly), 55.6% had higher prevalence of depressive symptomatology according to GDS-15. High figure compared with other studies that applied the same instrument and cut-off point (score greater than or equal to 6): 48.1% in Patras and Tripoli, Greece(29); 45.4% in Chihuahua, Mexico(30); In addition, 43% in Asunción, Paraguay(31); 31.1% in Jequié, Brazil(32); 29.5% in Antioquia, Colombia(12); 27,8% in Sri Lanka, Singapore(11); 19,7% in Guadalajara, Spain(18).
In Peru, studies published have reported in 2010 in AA.HH. “Viña Alta” located in La Molina district, in Lima; in 112 elderly, that 51.6% had depression with a score of five or more(24). In 2013, a study in 369 elderly from Breña district, Lima reported that 48.2% had depression with a score of six or more(23). In 2012, a study carried out in 72 people from a community of Masma Chicce (Junín) stated that 69.4% presented depression (25). It does not describe the score used in GDS-15(26). These percentages are slightly elevated if we compare them with our study. People probably had fewer chances to be attended by medical specialists (psychiatry, internal medicinal, geriatric, etc.), along with lack of consciousness of this geriatric syndrome in elderly and their relatives. The aforementioned would explain the limited use of mental health services in elderly from marginal urban areas, due to lack of mobility, transport, distance, travel time and expenses. Since it is usual that they live in the city outskirts.
ASSOCIATED FACTORS
Partner
Although we discovered the third part of elderly without partner (single, widow/widower, divorced) had risk of depressive symptomatology, we did not find statistical significance. The fact of not having a partner was a factor significantly associated in elderly from Pakistan(33), India(34) and Colombia(35). This may be due to somatic and emotional changes that experiment elderly without a partner and with a greater tendency to present depressive episodes in ageing. Lack of statistical significance in our study maybe due to limitation in sample size of study population. We recommend carrying out more studies that evaluate this topic.
Schooling
We discovered that the fact of no having completed their schooling was associated with risk of depressive symptomatology. This result was similar to those from previous studies in elderly from South Africa(8) , Colombia(12) , Brazil(17) , Nepal(20) and Mexico(20) . Level of education can influence in elderly’s quality of life, since it is part of learning experiences and cognitive reserve, so that a person with a higher level of education could be an adjuvant to face stressful situations avoiding that they disrupt his/her emotional state, thus diminishing risk of depression(36). In addition, we should implement strategies designed to improve level of education in elderly from marginal urban areas.
Working
In our study, elderly who did not work had higher prevalence of depression. Other studies performed in Pakistan(21) and India(37) . shared this finding. Study population in our research was poor. It is probable that elderly who did not have working life live a tenser and more stressful economic situation in their homes, being more likely to suffer from depression.
Limitations
Among limitations in this study, we can mention the small sample size. It is possible that in data collection period, we did not include every single elderly, since an actual record of the total of elderly from study place did not exist. Study population was limited to only one marginal urban area from Lima city. That is why we cannot extrapolate results to other cities of Peru. Our results allow giving a perspective of what could be happening in contexts like marginal urban communities. Using GDS-15 questionnaire as screening does not allow giving an accurate diagnosis of depression. Nevertheless, it is a short compressible instrument, and we have already used it in similar studies in Peru.
CONCLUSIONS
In short, we discovered five elderly out of ten had prevalence of depressive symptoms. Prevalence of depression was high in those elderly who did not complete their schooling and those who did not work. The findings of the study aim to reflect and to carry out more studies about mental health in elderly who live in marginal urban areas. Besides, regarding health workers, the findings aim to highlight the importance of diagnosing and treating depression in elderly who seek relief for their symptoms. Likewise, planning of strategies that enhance geriatric attention in primary care centers
Authorship contributions: The authors participated in the genesis of the idea, project design, data collection and interpretation, analysis of results and preparation of the manuscript of this research work.
Financing: Self-financed
Conflict of interest: The authors declare that they have no conflict of interest in the publication of this article.
Received: February 25, 2020
Approved: March 19, 2020
Correspondence: Christian Ponce Torres.
Address: Av. El corregidor 1531, Las Viñas, La Molina
Telephone: +51 995 473 883
Email: christianfpt01@gmail.com
BIBLIOGRAPHIC REFERENCES
