ORIGINAL PAPER
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2019 - Universidad Ricardo PalmaDOI 10.25176/RFMH.v20i2.2902
FACTORS ASSOCIATED WITH THE PERFORMANCE OF SELF-CARE ACTIVITIES IN DIABETIC PATIENTS IN THREE UCAYALI HOSPITALS
FACTORES ASOCIADOS A LA REALIZACIÓN DE ACTIVIDADES DE AUTOCUIDADO EN PACIENTES DIABÉTICOS EN TRES HOSPITALES DE UCAYALI
Jennifer Vilchez-Cornejo1, Luccio Romani2,3
, Silvia Reategui4
, Elice Gomez-Rojas4, Claudia Silva4
1Ucayali Assistance Network, EsSalud II Pucallpa Hospital, Ucayali-Peru.
2Faculty of Human Medicine, University of San Martín de Porres, Chiclayo-Peru.
3Scientific Society of Medical Students Veritas, Lima-Peru.
4Faculty of Human Medicine, National University of Ucayali, Ucayali-Peru.
ABSTRACT
Objective: To determine which are the factors associated with self-care activities in diabetic patients in three hospitals in the Ucayali region during 2017.
Methods: Analytical cross-sectional study, carried out in three hospitals in Ucayali in 2017. The survey self-administered had three sections that assess the general characteristics of the patients, knowledge through the diabetes knowledge questionnaire 24 (DKQ–24), the patient's attitude towards their disease using the diabetes attitude scale (DAS - 3) and Summary of Diabetes Self-Care Activities Measurement (SDSCA) to measure self-care practices.
Results: The study population consisted of 572 patients, 50.87% were female, the median age was 47 years old, 37.57% had a university degree. Inadequate self-care activities with respect to glycemic control and exercise were performed with 83.87% and 77.87% respectively. We consider that those who have adequate knowledge and have strict control to have adequate adherence to the diet of diabetic patients. Regarding exercise, it was possible to determine that there is a negative correlation with respect to the patient's illness time. Likewise, it was determined that patients with secondary, technical and university studies had a negative correlation with respect to glycemic control.
Conclusion: More than half of the patients carried out inadequate self-care activities. Furthermore, an adequate level of knowledge and strict control over their disease influence the patient's adherence to a good diet.
Keywords: Diabetes Mellitus; Self-Care; Health Knowledge; Attitudes; Practice (source: MeSH NLM).
s
RESUMEN
Objetivo: Determinar cuáles son los factores asociados a la realización de actividades de autocuidado en pacientes diabéticos en tres hospitales de la región de Ucayali durante el 2017.
Métodos: Estudio transversal analítico, realizado en tres hospitales en Ucayali en el 2017. La encuesta autoadministrada contó con tres secciones que evaluaban las características generales de los pacientes, los conocimientos a través del Diabetes Knowledge Questionnaire 24 (DKQ–24), la actitud del paciente frente a su enfermedad mediante la Diabetes Attitude Scale (DAS–3) y Summary of Diabetes Self Care Activities Measure (SDSCA) para medir las prácticas de autocuidado.
Resultados: La población de estudio estuvo conformada por 572 pacientes, el 50,87% correspondía al sexo femenino, la mediana de la edad fue de 47 años, el 37,57% tenía grado universitario. Se presentaron actividades de autocuidado inadecuadas con respecto al control glucémico y ejercicio con 83,87% y 77,87% respectivamente. Se observó que quienes contaron con un adecuado conocimiento y tuvieron un control estricto contaron con una adecuada adherencia respecto a la dieta de los pacientes diabéticos. Con respecto a realizar ejercicio se pudo determinar que existía una correlación negativa respecto al tiempo de enfermedad del paciente. Asimismo, se determinó que los pacientes con estudios secundarios, técnicos y universitarios presentaban una correlación negativa respecto al control glucémico.
Conclusión: Más de la mitad de los pacientes realizaban actividades de autocuidado inadecuados. Además, un adecuado nivel de conocimiento y un control estricto sobre su enfermedad influencian en la adherencia a una buena dieta del paciente.
Palabras Clave: Diabetes Mellitus; Autocuidado; Conocimientos; Actitudes y Práctica en Salud (fuente: DeCS BIREME).
Type II diabetes mellitus (DM2) is now considered a global public health problem. It is estimated that, globally, diabetes cases will reach 592 million in 2035, affecting 8.8% of the world’s population(1). Globally, an estimated 425 million adults suffer from diabetes mellitus (DM)(2). An increase in the prevalence of DM is expected to lead to an increase in the number of chronic and acute diseases in the population, directly affecting the quality of life, the demand for health services and the economy at the global level(1,2).
In Central and South America, more than 26 million people suffer from diabetes. It is estimated that the number of diabetic patients may increase to 693 million by 2045. There are currently reports of up to 352 million people with impaired glucose tolerance, with a high risk of developing DM. Low- and middle-income countries are also reported to bear almost 80% of the DM burden globally(3,4). In Peru, nearly 24,000 cases have been registered by 2018, with nearly 61.4% of those diagnosed with DM 2 being women(5).
The burden of diabetes decreases national health budgets, reduces productivity, slows economic growth, generates high costs for vulnerable households, and generates a large human burden, which is characterized by premature mortality and poor quality of life as a result of the complications of the disease, generating a significant economic impact both for countries and for health systems(6).
It has been demonstrated that education in DM on a continuous basis is a fundamental tool, both for the vulnerable population with risk factors and for those already suffering from this condition(6). Educating and informing the patient with DM, self-care measures and disease management, is an effective approach to achieve adequate adherence to treatment, the purpose of which is to control glycemic values and to reduce the possibility of both acute and chronic comorbidities and complications(7,8).
Self-care is defined as the set of intentional actions the person takes to control factors that may compromise his life and further development(9). The American Diabetes Association has proposed self-care as part of initial management and follow-up in patients with MD, and has been incorporated into clinical practice guidelines, due to its effectiveness, survival improvement, reduction of complications and achievement of therapeutic goals(7,8).
Therefore, the objective of this research is to determine the factors associated with the realization of self-care activities in diabetic patients in three hospitals in the Ucayali region during 2017.
METHODS
A cross-sectional analytical study was carried out in 2017 in three hospitals in the region of Ucayali, which correspond to the Social Health Insurance (Essalud Pucallpa Hospital II) and the Ministry of Health (Amazonian Hospital and Pucallpa Regional Hospital).
Population and sample
The initial study population consisted of 4,059 patients diagnosed with DM 2 distributed among 2531 patients at the Essalud II Hospital in Pucallpa, 522 at the Amazonian Hospital and 1,006 patients at the Regional Hospital, who came to the hospital for monitoring/ treatment and/or hospitalization. A sample size of 572 participants was calculated using the EPIDAT statistical programme with a 95% confidence level, a 5% margin of error and a 50% prevalence (0.5) A convenience sampling was carried out where participants were surveyed to the previously calculated sample size.
Patients diagnosed with DM 2 were considered within the study, within the hospitalization, emergency and/ or outpatient services, who were hemodynamically stable and agreed to participate in the study by signing their informed consent. Patients unable to complete the survey and/or who had to be referred from other centres outside the Ucayali region were excluded.
Procedure and variables
An anonymous self-administered survey was applied, covering the general characteristics of patients (age, sex, marital status and level of education), knowledge of DM 2, the patient’s attitude to DM 2 and self-care activities.
The Summary of Diabetes Self Care Activities Measure (SDSCA)(10) was used to measure self-care practices in DM, its version adapted to Spanish(11) has a Cronbach coefficient of 0.764. The instrument evaluates three main factors corresponding to diet, exercise and glucose control, the response scale being a Likert-type score ranging from 0 to 7 points depending on the number of days in the last week(11). For the interpretation of the results was delimited as a cut-off point of 3.5, being considered the answers minor or equal to this as inadequate.
The level of knowledge about diabetes was evaluated through the Diabetes Knowledge Questionnaire 24 (DKQ - 24)(12), a reduced version and in Spanish of the DKQ-60(13). which internal consistency corresponded to a Cronbach Alpha of 0.78(13). The current instrument consists of 24 items with alternatives of “yes”, “no” and “I don’t know”, giving a point to the correct answers and zero to the incorrect ones. The questionnaire has three sections that define basic knowledge about disease, glycaemic control and prevention of complications. For its evaluation and analysis the overall and corresponding score for each section was calculated by adding the score of the twenty-four reagents, with the highest scores indicating a higher level of knowledge about DM(12). For the purpose of this study, good knowledge was considered when more than 50% of correct answers (more than 12 points) were obtained.
Patient-related attitudes and motivations were measured through the Diabetes Attitude Scale (DAS - 3)(14), in its Spanish-adapted version(15) in a similar population, whose internal consistency had a Cronbach alpha coefficient of 0.74(15). This compound has five subscales which define the need for training, perception of the severity of diabetes mellitus, assessment of strict control, assessment of the psychosocial impact of diabetes mellitus and patient autonomy. It also consists of 33 items using a Likert scale with a maximum score of 5 and a minimum of 1, corresponding to "fully agreed" (5 points), "agreed" (4 points), "indifferent" (3 points), "disagreed" (2 points) or "totally disagreed" (1 point). However, the values of the scores were inverse (Items 2; 3; 7; 11; 13; 15; 16; 23; 26 and 28). Surveys that were not answered in more than 50% of the questions in one of the subscales were considered null(15). In addition, during our investigation was taken as a cut-off point, a score of less than or equal to 3 as inappropriate for each section.
Statistical analysis
Once the participants' data collection was completed, the data was recorded in a spreadsheet of the Microsoft Office Excel 2013 program. Being analyzed through the statistical package STATA version 15. For the descriptive statistics of the quantitative variables the Sknewness Kurtosis test (Sktest) was applied to find the normality of the distribution of the results, the variables that presented a normal distribution are expressed in mean and standard deviation (p>0.05) and those which are not, in median and interquartile ranges. The results were presented in tables and graphs, expressing the data obtained in nominal and percentage expression.
Finally, with respect to inferential statistics it was taken as variables dependent on the results of the subscales of the SDSCA (diet, exercise and glycaemic control) and as independent variables on age, level of education, level of knowledge about the disease obtained from DKQ-24 and the total DAS-3 score. For the analysis, generalized models were used applying crude prevalence (RPc) and adjusted prevalence (RPa) ratios and their 95% confidence intervals with respect to the self-care variables, considered as significant and p value < 0.05.
Ethical considerations
The collection of the information was carried out through a pollster who requested permission from the healthcare doctors of the nosocomias and subsequently the informed consent of the patients themselves. The ethical implications arising from international agreements on the subject, contained in the Helsinki Agreement, were respected. The protocol to this study was also approved by the Ethics Committee of the National University of Ucayali. In addition, informed consent was used and signed by each of the research participants.
RESULTS
The study population consisted of 572 patients, 50.87% (291) female, the median age was 47 years (interquartile ranges: 35 - 56). According to marital status 44.93% reported being married, 30.42% (174) living with their partner, 16.26% (93) single and 8.39% (48) reported being widowers. According to the degree of instruction reported, 37.57% (215) of the patients reported having a university level, 30.97% (177) secondary, 22.90% (131) technical, 6.64% (38) primary and 1.92% (11) reported not having any educational instruction. With regard to the type of hospital, 37.41% (214) of the population were treated at a hospital of the Ministry of Health and 62.59% (358) in EsSalud.
Within the clinical characteristics of the studied population, a median disease time of 3 years was shown (intercuartal ranges: 1 - 7). The most commonly used type of treatment was oral antidiabetic therapy with 70.80% (405), followed by insulin treatment with 19.41% (111) and a combination of both with 9.79% (56), with regular treatment follow-up reported in 83.69% (479) of the studied population. Among the comorbidities reported, 22.42% (128) patients reported hypertension (AHT), 9.81% (56) obesity 4.90% (28) Asthma, 3.50% Heart disease and 1.93% (11) COPD- Also 57.44% of patients reported no comorbidities.
Within the dimensions of the SDSCA self-care activities, more than half of the patients were found to have inadequate self-care activities with respect to glycemic control and exercise, reaching 83.87% (479) in glycemic control and 77.87% (446) in exercise; 63.64% (364) of the patients showed adequate self-care activities with respect to self-care in diet (Figure 1). According to the dimensions of attitudes to diabetes, reported through the DAS-3, inappropriate attitudes to diabetes were presented more frequently, reaching 63.64% (364) in the autonomy of diabetes, 69.93% (400) in the assessment of psychosocial impact, 44.06% (252) in the assessment of strict control, 51.59% (295) in the perception of gravity and 69.23% (396) in the need for training (Figure 2).
Within the dimensions of the diabetes knowledge scale (DKQ-24), 65.56% (375) of participants were found to have an inadequate level of knowledge, with an average score of 4.63 ± 1.81 in basic knowledge of the disease, 2.59 ± 1.31 in glycemic control, and 3.78 ± 1.47 in the prevention of complications, having a score of 11 ± 3.14 as average of the total score (Table 1).
With respect to inferential statistics, those with an adequate level of knowledge (Rpa: 1.31; 95% CI: 1.01- 1.48) predisposed to adherence to diet. Similarly, they presented a negative correlation, with the patient’s attitudes towards his illness (Rpa: 0.88; 95% CI: 0.85- 0.92) and the primary education grades (Rpa: 0.84; 95% CI: 0.98 - 0.99), technical studies (Rpa: 0.64; 95% CI: 0.49 - 0.76) and university studies (Rpa: 0.58; 95% CI: 0.51 - 0.80) statistically significant in the diet (Table 2).
With respect to adherence to exercise it was possible to determine that there was a negative correlation based on the patient’s disease time (RPa: 0.92 95% CI: 0.86 - 0.98) in addition to the patient’s predisposition to exercise by up to 21% (RPa: 1.21; 95% CI: 1.07 - 1.37) for the exercise. Finally, it was possible to determine a statistically significant association with respect to the level of education in those with secondary education (RPa: 0.20; 95% CI: 0.08 - 0.55), technical studies (RPa: 0.32; 95% CI: 0.12 - 0.82) and university studies (RPa: 0.39; 95% CI: 0.16 - 0.93) presenting a negative correlation with adherence to adequate glycemic control (Table 2).
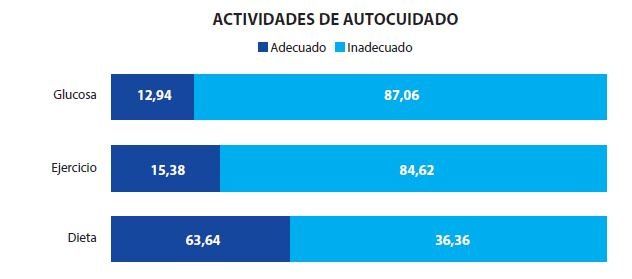
Figure 1. Dimensions of self-care activities in diabetic patients treated in three hospitals in the Peruvian Amazon.
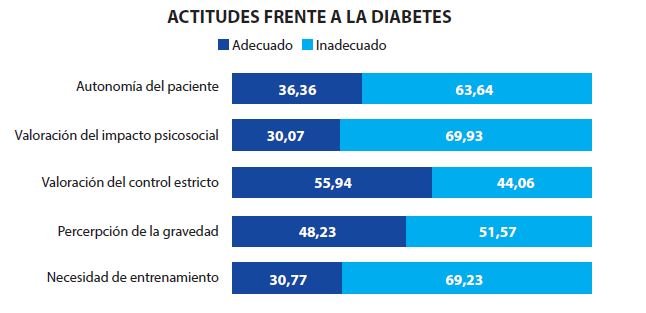
Figure 2. Dimensions of attitudes toward diabetes in diabetic patients treated in three hospitals in the Peruvian Amazon.
Table 1. Dimensions of the knowledge scale on diabetes (DKQ-24) in diabetic patients treated in three hospitals in the Peruvian Amazon.
|
Media |
Standard |
Rank |
||
|
Lower |
Upper |
|||
|
Basic knowledge of the disease |
4,63 |
1,81 |
0 |
9 |
|
Blood glucose control |
2,59 |
1,31 |
0 |
7 |
|
Prevention of complications |
3,78 |
1,47 |
0 |
7 |
|
Total score |
11 |
3.14 |
1 |
20 |
Table 2. Crude and adjusted analysis of the associated factors of self-care activities.
|
|
Diet |
Exercise |
Glucosa en sangre |
|||||||||
|
Bivariate analysis |
Multivariate analysis |
Bivariate analysis |
Multivariate analysis |
Bivariate analysis |
Multivariate analysis |
|||||||
|
|
RPc |
IC 95% |
RPa |
IC 95% |
RPc |
IC 95% |
RPa |
IC 95% |
RPc |
IC 95% |
RPa |
IC 95% |
|
Age |
0.99 | 0.99-1.00 | 0.99 | 0.98-0.99 | 0.99 | 0.97-1.00 | 1.00 | 0.99-1.02 | 1.00 | 0.98-1.01 | 1.00 | 0.98-1.02 |
| Degree of instruction | ||||||||||||
| None | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||||||
| Primary studies | 0.84 | 0.65-1.09 | 0.84 | 0.98-0.99 | 1.30 | 0.33-5.17 | 1.31 | 0.38-4.53 | 0.80 | 0.31-2.01 | 0.80 | 0.31-2.10 |
| Secondary studies | 0.75 | 0.60-0.92 | 0.61 | 0.66-1.08 | 0.40 | 0.10-1.57 | 0.45 | 0.13-1.54 | 0.19 | 0.07-0.48 | 0.20 | 0.08-0.55 |
| Technical studies | 0.68 | 0.54-0.86 | 0.64 | 0.49-0.76 | 0.97 | 0.26-3.57 | 0.85 | 0.26-2.72 | 0.34 | 0.14-0.83 | 0.32 | 0.12-0.82 |
| University studies | 0.63 | 0.51-0.79 | 0.58 | 0.51-0.80 | 1.05 | 0.29-3.79 | 0.99 | 0.32-3.08 | 0.40 | 0.17-0.93 | 0.39 | 0.16-0.93 |
| Sickness time | 1.01 | 1.01-1.02 | 1.02 | 0.46-0.72 | 0.91 | 0.86-0.97 | 0.92 | 0.86-0.98 | 0.96 | 0.90-1.03 | 0.96 | 0.89-1.03 |
| Knowledge level* | 1.38 | 1.43-1.79 | 1.31 | 1.01-1.48 | 0.80 | 0.52-1.22 | 1.26 | 0.80-2.00 | 0.66 | 0.40-1.08 | 0.88 | 0.50-1.57 |
| Attitudes** | 0.85 | 0.82-0.88 | 0.88 | 0.85-0.92 | 1.25 | 1.12-1.38 | 1.21 | 1.07-1.37 | 1.15 | 1.03-1.28 | 1.09 | 0.95-1.24 |
The promotion of self-care behaviour, understood as an activity initiated consciously and with a learning process, appropriate to a given situation and focused on a specific objective(16), is a nuclear element in the general approach to chronic diseases, and in the MD especially(17,18). In this article, we seek to determine the association between the socio-demographic characteristics, knowledge, attitudes and self-care activities that patients with DM have in the second level of care.
The main comorbidities reported in the patients were those who also had HTA and obesity, DM 2 has been found to be associated with a substantially increased risk of micro- and macrovascular events such as myocardial infarction and stroke(19). In addition, the development of AHT in diabetic patients is due to the appearance of proteinuria, impaired renal function and cardiovascular complications(20). Similarly, it has been determined that the main mechanisms for generating AHT have been due to insulin resistance hyperinsulinemia stimulated by sympathetic activity and renal sodium retention, a volume expansion secondary to elevated glucose levels and sodium reabsorption, followed by a vascular stiffness secondary to protein glycosylation(20,21).
Education about diabetes and managing diabetes care remain areas of interest and concern for health professionals and clinical researchers, even though a lot of research has been done in this area. Our results show that 65.56% of participants had inadequate levels of knowledge about diabetes, which is consistent with findings from other studies(22-24). Have adequate knowledge related to the etiology of diabetes, the symptoms present in high or low blood glucose levels, injury management, and the misconception that regular use of medicines is more important than dietary intake and exercise in diabetes control.
More than half of the diabetic patients performed inadequate self-care activities, results that highlight the need to improve self-care activities. Innovative approaches in education and self-care activities are necessary for lifestyle change. Flexible self-care interventions that can respond to an individual, unique, daily and cultural approach are recommended(25).
The attitude to the disease is a key point in determining behavior patterns, representing a predisposition for the adoption of self-care actions, favoring the reduction of stress associated with the disease, greater adherence to treatment, improved self-esteem and a more positive perception of health(26). The results of the application of DAS-3 in our study, reported more frequently inadequate attitudes towards DM, thus demonstrating the need to develop teaching activities and health education practices, focused on strengthening the active attitude towards the disease, since it is related to improving the self-management of the disease, improving the coexistence of the person with his condition(25,27,28).
A similar study(29), identified the attitude that most diabetic patients can develop to their disease, in contrast to our study, where it is reflected that only a small part of them see the need to change their eating habits. In our study, it was observed that an adequate level of knowledge, in addition to giving patients strict control over recommendations about their illness, led to substantial improvement in their diet, This could be due to the fact that the majority of patients who start with DM2 do not consider diet as a better habit in their new lifestyle, as the level of knowledge it brings is initially estimated to be poor(30). The strict control of patients coincides according to several researchers(31-33), in the interventions based to improve behavior in their diet, these results, beneficial at the beginning of the treatment, especially in those patients who were willing to make changes to their diet, which would explain why when they adapt properly they have good practices..
The limitations presented during the investigation were the rejection rate of diabetic patients surveyed during outpatient, hospitalization and/or emergency, in addition the lack of a case study control and/or longitudinal in order to delimit the causality between the variables. Our research recommends improving the selfcare activities within diabetic patients, strengthening the programs in which diabetic patients are found, as well as seeking strategies to carry out an accompaniment by specialized units (nutrition, psychology, endocrinology) which can provide better tools for optimal self-care.
CONCLUSION
Finally, it can be concluded that more than half of the patients performed inadequate self-care activities. In addition, an adequate level of knowledge and strict control over your illness influence adherence to a good diet of the patient.
Acknowledgments: The authors of the present investigation wish to thank Luz Vanessa Valdivia Martell for the collection of the data and to be part of the initial versions of this investigation.
Authorship contributions: The authors participated in the genesis of the idea, project design, data collection and interpretation, analysis of results and preparation of the manuscript of the present research work.
Funding: This research is partially funded by the Camisea Socioeconomic Development Fund (FOCAM) of the Faculty of Human Medicine corresponding to the National University of Ucayali during 2017.
Conflict of interest: This research was part of the undergraduate thesis of the medical surgeon Claudia Cristina Silva Bardales. However, the authors declare that they have no personal conflict of interest.
Received: March 12, 2020
Approved: March 30, 2020
Correspondence: Jennifer Steffany Vilchez Cornejo.
Address: Jr. Ramón Castilla 159 Mz E Lote 11, Ucayali-Perú.
Telephone: 961 506 868
E-mail: j.vilchezcornejo@gmail.com
BIBLIOGRAPHIC REFERENCES
