ARTICULO ORIGINAL
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2021 - Universidad Ricardo Palma10.25176/RFMH.v21i2.3608
WORK CONDITIONS AND PERSONAL PROTECTIVE EQUIPMENT AGAINST COVID-19 IN HEALTH PERSONNEL, LIMA-PERU
CONDICIONES LABORALES Y EQUIPOS DE PROTECCIÓN PERSONAL CONTRA EL COVID-19 EN PERSONAL DE SALUD, LIMA-PERÚ
Jarvis Giusseppe Raraz-Vidal(1,a), Henry Lowell Allpas-Gomez(1,a,b,c), Flor Karina Torres-Salome(2,d), Wenner Manuel Cabrera-Patiño(3,a), Lilian Maria Alcántara-Leyva(3,a), Rafael Paolo Ramos-Gómez(3,a), Flor Karina Aldea-Chihuantito(3,a), Viviana Colona-Risco(4,d), Omar Baldomero Raraz-Vidal (1)
1 Miembro de European Association of Science Editors; Universidad Nacional Hermilio Valdizán,
Lima-Perú.
2Facultad de Enfermería; Universidad Nacional del Callao-Perú.
3 Facultad de Medicina Humana; Universidad Nacional Mayor de San Marcos-Perú.
4Facultad de Enfermería; Universidad Norbert Wiener, Lima-Perú.
aMedical Surgeon.
bMaster in Occupational Health.
cInternal Medicine.
dBachelor in Nursing.
ABSTRACT
Objective: To determine the association between working conditions and access to personal protective equipment (PPE) in health personnel in the city of Lima-Perú. Methods: Descriptive, cross-sectional and analytical study. The sample was of 271 respondents virtually in the city of Lima, who met the selection criteria, captured between 07/09/2020 to 08/09/2020. The data collection instrument was validated by expert judgment with a score> 80% (content validity). An analysis was carried out with the generalized linear model of the Poisson family, log link function, robust models with fit. A statistically significant value of p <0.05 was considered. Results: The 55% of health personnel (HCP) worked more than 12 hours and only 53% received one PPE per day of work. 40% of the HCP almost never received a mask. In the multivariate analysis, the SP with ages <26 years (p=0.00) and from 26 to 55 years (p=0.00) received an incomplete PPE. The HCPs who did not have an employment relationship with the institution (p=0.02) received a mask on few occasions. Conclusion: Health personnel under the age of 56 rarely received PPE. When they work without an employment relationship, they sometimes receive a mask.
Key words: Personal protective equipment; COVID-19; Health personnel; Organization at work and occupational health (Source: DeCS BIREME).
RESUMEN
Objetivo: Determinar la asociación entre las condiciones laborales y el acceso al equipo de protección personal (EPP) en el personal de salud de la ciudad de Lima-Perú. Métodos: Estudio descriptivo, transversal y analítico. La muestra fue de 271 encuestados virtualmente en la ciudad de Lima, que cumplieron los criterios de selección, captados entre el 09/07/2020 al 09/08/2020. El instrumento de recolección de datos fue validado por juicio de expertos con un puntaje >80% (validez de contenido). Se realizó un análisis con el modelo lineal generalizado de familia Poisson, función de enlace log, modelos robustos con ajuste. Se consideró un valor estadísticamente significativo de p<0,05. Resultados: El 55% del personal de salud (PS) trabajaron más de 12 horas y solo el 53% recibieron un EPP por día de trabajo. El 40% del PS casi nunca recibió una mascarilla. En el análisis multivariado el PS con edades <26 años (p=0,00) y de 26 a 55 años (p=0,00) recibieron un EPP incompleto. Los PS que no tenían un vínculo laboral con la institución (p=0,02) recibieron una mascarilla en pocas oportunidades. Conclusión: El personal de la salud menores de 56 años recibieron con poca frecuencia un EPP. Cuando trabajan sin un vínculo laboral reciben algunas veces una mascarilla.
Palabras Claves: Equipo de protección personal, COVID-19, personal de salud, condiciones laborales y salud ocupacional (Fuente: DeCS BIREME).
INTRODUCTION
SARS-CoV-2 (COVID-19) spread worldwide, being classified as a pandemic by the World Health Organization
(WHO) in March 2020 and until that date no effective drugs or vaccines are available to combat it. Cases
of COVID-19 continue to increase, especially in the American continent, which has increased the need for
frontline health professionals in both public and private institutions, even working long hours.
(1,2) Because of these frontline health workers have a high
risk of infection, this contributes to a greater spread of the disease, (3,4) representing up to 20% of COVID-19 cases in a country. (5) The proper use of N95 or similar masks can reduce the possibility of
contracting COVID-19 by 64% to 75%. (6) Peru is no stranger to this reality
and is one of the main countries with more cases of COVID-19 according to reports from Johns Hopkins
University. (7)
The Centers for Disease Control and Prevention (CDC) and WHO recommend non-pharmacological
measures such as: hygiene, disinfection, early detection and use of personal protective equipment (PPE)
such as non-sterile and sterile gloves, N95 / PPF2 mask, face protector, protective goggles, disposable
aprons, disposable clothing, among others. (8-10) However, there was a
worldwide shortage of PPE, especially masks, due to the high demand from health institutions and the
population, in addition to the interruption of the supply chain of medical supplies. (9,11) due to this great need, health professionals reuse
(11) and even refurbish an PPE of materials not recommended for safe
protection, (12) putting their health at risk. The risk of infection
increases when the worker works in the Intensive Care Unit (ICU) area, or COVID-19 wards, especially
when the hospital does not have an efficient system of air replacements. As a result, the health
professional may contract COVID-19 disease and need to be hospitalized, even use mechanical ventilation
in the ICU or lose his life, figures that increased as the problem of access to PPE worsened. (15)
In hospitals, biosafety measures must be strict. These guidelines suggest a mandatory minimum
ratio of personal protective equipment according to the level of risk, previously assessed by the
occupational health and safety area, which suggests the type of PPE according to the occupational risk.
(8,16) there is poor implementation of occupational safety and
health policies, especially in the health systems of developing countries. And they have weak health
systems. (17,18)
The organisms that watch over occupational health recommend that access to PPE should be
ensured, improving working conditions integrated with the prevention measures established in the
organizational plans against COVID-19. (8,16,19)
Therefore, the study aimed to determine the association between working conditions and access to
PPE for health personnel in the city of Lima-Perú.
METHODS
Design and study area
The study design was: descriptive, cross-sectional and analytical. He was executed between July 9 and August 9, 2020. A survey was conducted of the health personnel of the city of Lima.
Population and sample
Virtually a survey was sent to 753 people ≥ 18 years of age, through social networks in order to
reach all the different reference hospitals in the city of Lima, which were distributed in the districts
of: Villa el Salvador, La Victoria, Ate, San Martin de Porras, Breña, el Agustino, Lince, Miraflores,
Independencia, San Juan de Lurigancho and Callao. Of which 553 were answered by health personnel, 230
did not meet the selection criteria (surveys of people who did not want to participate in the study,
those under 18 years of age, health personnel who did not work directly with patients diagnosed with
COVID-19, foreigners, primary care, from other cities, inconsistent or partial answers), so that in the
end only 271 surveys remained.
The sample was not random, it had a snowball sampling, so the participants shared the link of
the virtual survey to their health contacts (friends, family or coworkers), through social networks such
as "Facebook, Telegram and WhatsApp".
To estimate the association between working conditions and access to personal protective
equipment, the theoretical bases were reviewed and a virtual survey was constructed. The first version
of the survey contained 24 questions, with dichotomous, polytomous, multiple choice or data-filling
alternatives.
Variables and tools
The main variables of the study were: PPE access; receives mask, age, employment relationship, area of work, occupational group, working hours and years on the workplace.
The survey was validated by 13 experts (physicians, nurses, pharmaceutical chemist, nutritionist, medical technologist, health professional, Occupational Medicine and Health Management) with which it reached a score of over 80% in content validity. Subsequently, a pilot study of the virtual survey was conducted with 36 people to improve internal validity, with the results obtained 8 questions were removed and only 17 remained. The survey had the following parts: the first were sociodemographic data consisting of 4 questions on (age, gender, city of residence and occupation); The second part corresponded to working conditions which had 6 questions (type of contract, institution where you work, level of attention of the workplace, profession, area of the hospital where you work, hours of work per shift and years of work experience); The third part asked about personal protective equipment with 4 questions (types of PPE you received from your employer, if you received a complete/incomplete PPE, how many days you were given an PPE and how many days you were given an N95 mask) and the fourth part contained questions that were used to apply the selection or adjustment criteria of the statistical analysis (works directly with a patient diagnosed with COVID-19, at your workplace perform screening for COVID-19 and you were diagnosed with COVID-19).
Procedures
Due to the context of the current pandemic, a virtual survey was conducted using a Google Drive sheet. The questions validated by expert judgment were appropriate in the Google Drive form and subsequently a pilot study was conducted. The message sent by social networks "Facebook, Telegram and WhatsApp" contained a brief description of: the purpose of the study, that the survey would be anonymous and the indication if you wanted to participate in the study "click on link of the virtual survey". When entering the survey, a message would appear "whether or not I wanted to be part of the study," if they marked "no" the survey ended and if they marked "yes" they continued with the development of the questions. In order to obtain the largest number of respondents, the link was shared to one or more health workers from the districts of Lima Norte, Centro, Este, Sur and Callao. Also influential people contributed in sharing and recommending that the link is not a virus. The Google Drive program stored all the answers in real time in an Excel format, then worked with the database according to the selection criteria, for the second time the information was corroborated to rule out any error, then coded the variables according to the objectives of the study and finally exported the data to the statistical program SPSS version 24.
Ethical aspects
The ethical principles in research according to the Helsinki Norms were respected, participation was voluntary, anonymous and the data were treated confidentially.
Statistical analysis
A descriptive and analytical study was carried out according to the objectives of the study. For the
descriptive analysis we used percentages and frequencies for polytomous variables. Tables and graphs
were also created according to the type of variable. With the Kolmogórov-Smirnov test, we determined
that the sample did not have a normal distribution (p=0.00).
In the first analysis, chi-square was used for categorical variables. Next, multivariate analysis was
performed with generalized linear models with Poisson family, log link function and robust models. This
was adjusted for gender and COVID-19 diagnosis. A statistically significant value of p<0.05 and a
confidence interval of 95% was considered.
RESULTS
Of all health personnel, 271 met the selection criteria. The female population was more representative
(71%) in the study. The mean age of the total participants was 42 (+10.10 years), with an age range from
21 to 70 years.
The age group with the largest population was 31 to 45 years, followed by 46 to 55 years. The
majority of the male gender worked as physician; the majority of the female gender were nurses. (Table 1)
Table 1. Occupational group according to age group and gender in health personnel.
| Occupational group | N | % | Age group (years) | Gender | |||||
|---|---|---|---|---|---|---|---|---|---|
| < 31 | 31 a 45 | 46 a 55 | 56 a 64 | > 64 | M | F | |||
| Medical specialist | 29,2 | 2 | 40 | 26 | 8 | 3 | 43 | 36 | |
| Resident physician | 32 | 11,8 | 15 | 15 | 2 | 0 | 0 | 14 | 18 |
| General physician | 9 | 3,3 | 1 | 6 | 2 | 0 | 0 | 2 | 7 |
| Nurse practitioner | 60 | 22,1 | 1 | 25 | 21 | 13 | 0 | 2 | 58 |
| General nurse | 46 | 17,0 | 11 | 28 | 6 | 1 | 0 | 7 | 39 |
| Laboratory personnel | 11 | 4,1 | 4 | 3 | 4 | 0 | 0 | 4 | 7 |
| Other health professions | 18 | 6,6 | 1 | 7 | 4 | 6 | 0 | 4 | 14 |
Multivariate analysis found that the health professional who belonged to the age group <26 years was more likely to receive an incomplete PPE (PR: 25.3; 95%CI: 23.9-26.7, p value=0.00), compared to workers aged 56 to 64; Similarly, the age group of 26 to 55 years received more frequently an incomplete PPE (PR: 24.8; 95%CI: 24.1-25.5, p value= 0.00), compared to workers aged 56 to 64; In both age groups the statistical model was adjusted for: type of contract, level of the workplace, area of work, profession, hours of work per shift, years of work experience, gender and the reference on the COVID-19 diagnosis. The health professional who did not have a contract (temporary without employment) received a mask less frequently (RP: 0.75; 95%CI: 0.14-0.9, p value= 0.02), compared to those who had permanent employment; This crossover was adjusted for age group, workplace level, area of work, profession, working hours per shift, years of work experience, gender, and COVID-19 diagnostic reference. The provision of incomplete PPE or not receiving a mask per work shift had no association with workplace level, occupation, hours of work per shift, and years on the workplace. (Table 2)
Table 2. Multivariate analysis of the factors associated with receiving incomplete PPE and not receiving a mask in the health professional.
| n | % | Receives a PPE incomplete | RP | 95% IC | P | Receives mask | RP | 95% CI | P | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| YES | NO | NO | YES | |||||||||
| Age | ||||||||||||
| <26 years | 5 | 1.8 | 2 | 3 | 25.3 | 23.9 -26.7 | O,OO | 4 | 1 | not significant | ||
| 26 to 55 years | 235 | 86.7 | 156 | 79 | 24.8 | 24.1 -25.5 | O,OO | 142 | 93 | not significant | ||
| 56 to 64 years | 28 | 10.3 | 18 | 10 | Reference | 19 | 9 | Reference | ||||
| >64 years | 3 | 1.1 | 3 | 0 | NA | 2 | 1 | NA | ||||
| Employment relationship | ||||||||||||
| Permanent (appointed) | 87 | 32.1 | 60 | 27 | not significant | 56 | 31 | not significant | ||||
| Temporary direct link* | 51 | 18.8 | 34 | 17 | not significant | 34 | 17 | not significant | ||||
| Temporary indirect link** | 21 | 7.7 | 14 | 7 | not significant | 8 | 13 | 0.75 | 0.14 - 0.9 | 0.02 | ||
| Temporary no link | 112 | 41.3 | 71 | 41 | Reference | 69 | 43 | Reference | ||||
| Area of work | ||||||||||||
| Physician’s office o topic | 17 | 6.3 | 17 | 0 | NA | 8 | 9 | Reference | ||||
| Diagnostic imaging | 13 | 4.8 | 12 | 1 | not significant | 5 | 8 | not significant | ||||
| Emergency | 68 | 25.1 | 45 | 23 | not significant | 45 | 23 | not significant | ||||
| Hospitalization | 70 | 25.8 | 46 | 24 | Reference | 38 | 32 | not significant | ||||
| Clinical Laboratory | 9 | 3.3 | 5 | 4 | not significant | 6 | 3 | not significant | ||||
| Clinical Pathology | 6 | 2.2 | 6 | 0 | NA | 2 | 4 | not significant | ||||
| ICU | 32 | 11.8 | 16 | 16 | not significant | 25 | 7 | not significant | ||||
| Low exposure to COVID-19& | 56 | 20.7 | 32 | 24 | NA | 38 | 18 | not significant | ||||
| Occupational group | ||||||||||||
| Medical specialist | 79 | 29.2 | 52 | 27 | not significant | 53 | 26 | not significant | ||||
| Resident physician | 9 | 3.3 | 7 | 2 | not significant | 6 | 3 | not significant | ||||
| General physician | 32 | 11.8 | 29 | 3 | not significant | 16 | 16 | not significant | ||||
| Practitioner nurse | 60 | 22.1 | 35 | 25 | not significant | 35 | 25 | not significant | ||||
| General nurse | 46 | 17.0 | 25 | 21 | not significant | 31 | 15 | not significant | ||||
| Laboratory personnel | 11 | 4.1 | 7 | 4 | Reference | 5 | 6 | Reference | ||||
| Nursing Technician | 16 | 5.9 | 13 | 3 | not significant | 11 | 5 | not significant | ||||
| Other health professions | 18 | 6.6 | 11 | 7 | not significant | 10 | 8 | not significant | ||||
| Hours worked per shift | ||||||||||||
| 6 hours | 52 | 19.2 | 29 | 23 | not significant | 39 | 13 | not significant | ||||
| 8 hours | 18 | 6.6 | 9 | 9 | not significant | 12 | 6 | not significant | ||||
| 12 hours | 149 | 55.0 | 87 | 62 | not significant | 100 | 49 | not significant | ||||
| 24 hours | 52 | 19.2 | 42 | 10 | Reference | 28 | 24 | Reference | ||||
| Years on the workplace | ||||||||||||
| <1 year | 11 | 41 | 5 | 6 | not significant | 10 | 1 | not significant | ||||
| 2 to 5 years | 63 | 23,2 | 40 | 23 | not significant | 36 | 27 | not significant | ||||
| 6 to 10 years | 50 | 18,5 | 39 | 11 | not significant | 33 | 17 | not significant | ||||
| 11 to 29 years | 127 | 46,9 | 80 | 47 | not significant | 75 | 52 | not significant | ||||
| >30 years | 20 | 7,4 | 15 | 5 | Reference | 13 | 7 | Reference | ||||
|
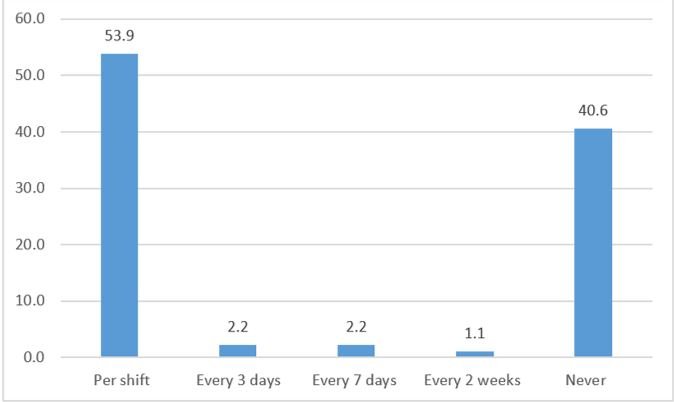
53.9% of the study population reported that they receive their PPE for each work shift, 40.6% reported that they never received PPE for the care of patients with COVID-19. (Figure 1)
|
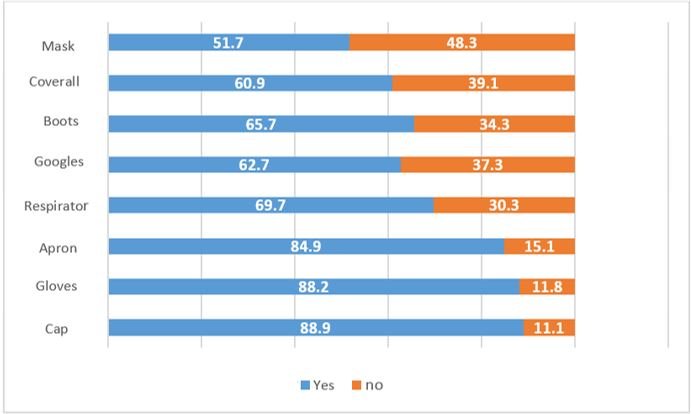
The study population reports that the PPE they receive most from their employer are: cap (88.9%), gloves (88.2%) and apron (84.9%). (Figure 2)
|
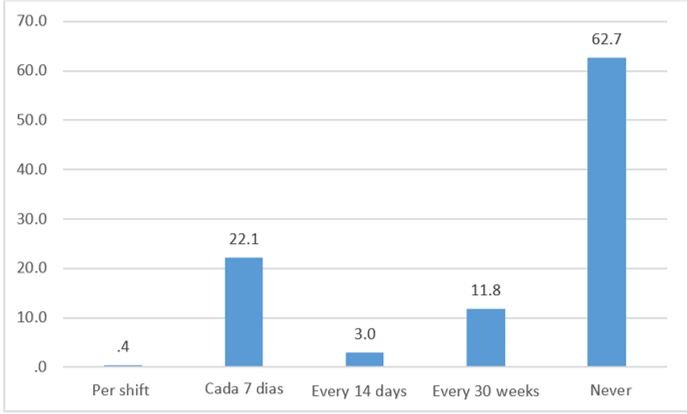
62.7% of health personnel reported that they were never given an N95 mask and only 0.5% received one N95 mask per shift. (Figure 3)
|
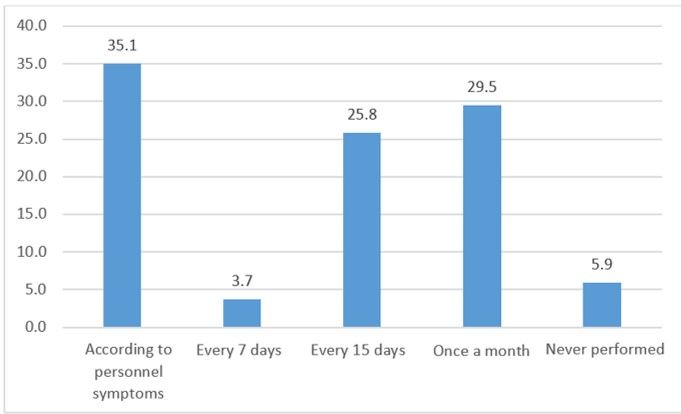
Health personnel reported that they usually take at least one rapid test if: they present symptoms of COVID-19 (35.1%), monthly control (29.5%), every 15 days (25.8%) and some never take them (5.9%). (Figure 4)
DISCUSION
In our study, 55% of the health personnel reported having received personal protective equipment (PPE)
for each work shift. Lack of PPE provision may be due to pandemic shortages and high demand at different
levels of health care globally. (9,12) Another explanation is
the interruption in the supply chain of medical supplies, insufficient production to meet market demand
for PPE in Peru.
It has been reported that when the PPE is reduced, health personnel purchase their own personal
protective equipment, reuse or adapt with other materials not certified for such work, thereby
increasing the risk of contracting the SARS-CoV-2 virus. (12) This scenario
would explain why frontline health personnel can represent from 10% to 20% of all infected cases by this
disease in a country. (5)
Our results coincide with a study in Latin America, where health professionals had limited
access to PPE such as: face protector, mask, disposable gown, and among others. (2) This despite the WHO recommended personal protection equipment as a
priority to work in COVID-19 patient care.
Health personnel also carry out activities outside the hospital, such as: home visits,
evaluation to determine epidemiological maps, etc.; Transit through these places does not guarantee
compliance with the administrative and security controls that are implemented in hospitals, especially
in a pandemic. (20) For the above reasons, health personnel are a vulnerable
population in this pandemic; providing personal protective equipment is an obligation of the employer,
whether state or private, thereby reducing the risk of contracting the disease, with the consequent
reduction of staff insecurity to provide care to a suspected or confirmed COVID-19 patient. (21)
Our study reports that incomplete personal protective equipment was given to health personnel
under 56 years of age; this finding may explain why priority was given to the delivery of complete PPE
to health personnel at greater risk of vulnerability when contracting COVID-19, also health personnel ≥
56 years (11%) were working in different institutions. One study found that among hospitalized health
professionals who died of COVID-19, mortality doubled between the ages of 50 and 59, quadrupled between
the ages of 60 and 69, and was 12 times higher after age 70 compared with younger patients. (3)
The risk of contracting COVID-19 has been exacerbated by inadequate provision of personal
protective equipment. (22) This information is consistent with another
epidemic of severe acute respiratory syndrome (SARS), where inadequate PPE use was associated with
increased risk of the disease. (23)
In the study, half of the health personnel worked more than 12 hours per shift caring for
patients diagnosed with COVID-19. The extension of working hours may be due to cover shifts of staff in
quarantine due to COVID-19, staff shortages due to high demand and comorbidity leave. All this added to
a lack of a ventilation system with air exchange, which can increase the risk of contracting COVID-19,
since it is known that the virus is transmitted by air. (4,14)
Studies have clearly shown that the severity of COVID-19 is directly proportional to the viral load in
the airways. (14) This explains why there are a large number of physicians
infected and killed by COVID-19 in Peru, in the different services, such as the intensive care unit,
hospitalization and others. (15) Here the importance of caring for health
personnel and providing them with the necessary PPE. (24)
In addition, there are studies showing that long working hours affect health, suggesting an
increased risk of cardiovascular disease and cancer. (24,25)
In addition, excessively long working hours (> 12 hours) also deteriorate the mental health status of
workers, generating symptoms of anxiety, depression, and sleep disorders. (26) A study in China showed that, during the COVID-19 outbreak, sleep
disturbance was highly prevalent in health professionals. (27)
50.9% of respondents reported that they were almost never given an N95 respirator per shift.
These results can be explained by the growing need to have a greater number of N95 respirators, the high
demand for respirators at different levels of the health sector, the increase in the purchase by the
population triggered the shortage of this medical input, (9,12) to this was added the increase in prices of up to ten times its usual
value by suppliers, leading to a restricted and high cost good. Our results coincide with the study
carried out on health professionals in Latin America, where only 56% of the health professionals who
attended patients diagnosed with COVID-19, had access to N95 respirators, the hospital filled this gap
by assigning surgical masks to its workers. (2) Surgical masks are not
recommended as respiratory protection for jobs with high exposure to COVID-19. (28) It is evident that the FFP2 respirator, followed by the N95 respirator
meet the requirements for filtration of small airborne particles, another advantage of these respirators
is the tight fit to the user's face being more effective than surgical masks in reducing exposure to
COVID-19. (13,28,29) In a study conducted on
N95 respirators, their use showed efficient blocking against SARS-CoV-2 virus particles. (30) Therefore in health professionals, respirators such as FPP2 or N95 are
very necessary to use them for adequate protection against this disease, without leaving aside frequent
hand washing. (31)
The results of the study show that neither the profession nor the area where health personnel
work has a difference in access to PPE. This could be explained due to the shortage of personal
protective equipment in the global context caused by the pandemic. (9,10) At least the purchase of N95 respirators should be prioritized for health
personnel working in areas of higher risk of exposure to COVID-19, (3,14) since the main route of transmission of this disease is the air and the
N95 respirator has been shown to reduce the rate of infection by COVID-19. (6)
A study described the levels of risk in health professionals who worked with COVID-19 patients, the
areas of high exposure to this disease were: hospitalization and internal medicine, even reaching a
higher average of this disease when compared to other areas or hospital services, especially nurses,
followed by physicians. (32)
Our results show that about half of the health professionals (41%) did not have an employment
contract and this group was assigned sometimes N95 respirator. This would be explained by the abrupt
demand for jobs to cover the growing need to care for COVID-19 patients, labor informality increased in
the health sector. This problem of informal employment leads to inequalities and inequity. Currently,
the Peruvian state does not have the necessary logistics system to monitor compliance with labor laws,
and many companies take advantage of this situation. (33)
Our study agrees with the results of research conducted on health professionals that included
Hispanics, Asians and ethnic minorities, they did not have adequate PPE despite working in the area of
COVID-19 patient care; They even report that 23% of the health personnel reported that they reused the
PPE. (34) In addition, they had much lower wages compared to workers with a
formal contract. (35)
As described above, the incipient development of occupational health areas in hospitals is still
an Achilles’ heel in Peru and other Latin American countries. (15,18) In the context of the pandemic in Peru, the Ministry of Health published
a regulation (Ministerial Resolution N° 448 - MINSA), focused on guidelines for the surveillance,
prevention and control of workers' health in the context of COVID-19, It describes a worker's risk
factors against COVID-19, based on age and comorbidities. As well as using PPE according to the level of
risk of exposure to COVID-19 at the workplace. Health personnel are classified as medium and high risk
of exposure to COVID-19. (16) The ILO, WHO and CDC also recommend that health
professionals should use an appropriate PPE, since the risk of exposure to SARS-CoV-2 is frequent during
routine tasks performed. (8,10,36) With
published evidence in the world and standards in Peru, the occupational health areas of hospitals have
the duty to implement occupational health policies to reduce the morbidity and mortality of this
pandemic among health professionals. Prevention and promotion of health in the workplace improves
productivity, reduces absenteeism due to illness, strengthens safety and improves job satisfaction.
Regarding the limitations of this research, we found only one multicenter study in Latin America
on the use of personal protective equipment, but it does not specify information about Peru. In this
study, most of the health personnel who responded to the survey were women from different health areas;
however, in the multivariate analysis, the statistical adjustment was made.
The sample size does not represent the population of the city of Lima (Peru) even though there
were respondents from different districts of the city, so it cannot be extrapolated to the entire
population of Lima.
The information generated by the virtual survey to carry out the research is considered as a
self-report, which could suffer from a bias.
It is recommended for future research to carry out studies on the effectiveness of the use of
PPE in reducing the number of people infected by COVID-19 in health workers according to hospital level.
CONCLUSION
Young health personnel and those under 56 years of age infrequently received full personal protective equipment. Health personnel without a work contract less frequently received an N95 mask. Finally, only half of the health personnel reported receiving personal protective equipment for each work shift.
Author contributions:Jarvis G. Raraz-Vidal: Conceptualization, methodology, software,
validation, formal analysis, research, resources, data curation, writing, original draft,
writing: review and edit, visualization, supervision, project management, fund acquisition
(self-funded)
Henry L. Allpas-Gomez: Conceptualization, methodology, research, writing, original draft,
writing: revising and editing, visualization.
Flor K. Torres Salome: Conceptualization, resources, writing, visualization, original draft,
writing: revising and editing.
Wenner M. Cabrera Patiño: Conceptualization, resources, writing, visualization, writing:
proofreading and editing.
Lilian M. Alcántara Leyva: Conception of the idea, data collection, writing and approval of the
final manuscript.
Flor K. Aldea Chihuantito: Conception of the idea, data collection, writing, original draft and
approval of the final manuscript.
Rafael P. Ramos Gómez: Conception of the idea, data collection, writing and approval of the
final manuscript.
Viviana Colona Risco: Conception of the idea, data collection, writing and approval of the final
manuscript.
Omar B. Raraz-Vidal: Conceptualization, methodology, validation, writing, original draft,
writing: revising and editing, visualization and project management.
Funding: Self-funded.
Conflict of interest: The authors declare no conflict of interest for the development of
the research.
Received: January 13, 2021
Approved: February 15, 2021
Correspondence: Jarvis Giusseppe Raraz-Vidal.
Address: Av. Metropolitana Nº 345, Ate, Lima-Perú.
Telephone: +51 952062495
E-mail: jarviervidal@hotmail.com
REFERENCES
