ORIGINAL ARTICLE
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2024 - Universidad Ricardo Palma10.25176/RFMH.v24i1.6338
ASSOCIATED FACTORS WITH TREATMENT ADHERENCE IN CHILDREN AGED 1 TO 3 YEARS: A STUDY AT THE “SEÑOR DE LOS MILAGROS” HEALTH CENTER, HUAYCAN – ATE
FACTORES ASOCIADOS A LA ADHERENCIA AL TRATAMIENTO EN NIÑOS DE 1 A 3 AÑOS. UN ESTUDIO EN EL CENTRO DE SALUD “SEÑOR DE LOS MILAGROS” HUAYCAN – ATE
Imelda Lourdes Oscanoa Huamán
 1,a
1,a
Luis Enrique Podestá Gavilano
1,b
1 “Señor de los Milagros” Health Center, Huaycán. Lima, Peru.
1 Hospital II Vitarte EsSalud. Lima, Peru
a Assistant Physician at the Health Center
b MD, General Surgeon
ABSTRACT
Objective: To determine the factors associated with treatment adherence in children aged 1 to 3
years at the "Señor de los Milagros" Health Center in Huaycán – Ate.
Methods: This observational, retrospective, cross-sectional study investigated adherence to
anti-anemic treatment in 169 children aged 1 to 3 years diagnosed with anemia, selected from an initial
group of 300. Using a data collection form, variables covering maternal, sociocultural, treatment, and
health system aspects were evaluated through bivariate analysis and Pearson's Chi-square test.
Results: The results highlighted low treatment adherence, with only 4.7% of children showing high
adherence and 15.4% demonstrating non-adherence. Higher adherence was observed in mothers with secondary
education, homemakers, and those living with their partners. Factors such as receiving understandable
information, respectful treatment, and proximity to the health center positively influenced adherence.
Conclusion: There is a significant association between adherence to anti-anemic treatment and
maternal, sociocultural, and treatment-related factors (p<0.05), suggesting that improving
communication, socioeconomic support, and accessibility could enhance therapeutic adherence.
Keywords: Anemia, treatment adherence, factors. (Source: MeSH NLM).
RESUMEN
Objetivo: Determinar los factores asociados a la adherencia al tratamiento en niños de 1 a 3 años
en el centro de salud “Señor de los Milagros” Huaycán – Ate.
Métodos: Este estudio observacional, retrospectivo y de corte transversal investigó la adherencia
al tratamiento antianémico en 169 niños de 1 a 3 años diagnosticados con anemia, seleccionados de un
grupo inicial de 300. Utilizando un formulario de recolección de datos, se evaluaron variables que
abarcaban aspectos maternos, socioculturales, de tratamiento y del sistema de salud, mediante análisis
bivariado y la prueba de Chi-cuadrado de Pearson.
Resultados: Los resultados destacaron una baja adherencia al tratamiento, con solo el 4,7% de los
niños mostrando alta adherencia y un 15,4% presentando no adherencia. Se observó una mayor adherencia en
madres con educación secundaria, amas de casa y en convivencia con su pareja. Factores como la recepción
de información comprensible, el trato respetuoso y la proximidad al centro de salud influían
positivamente en la adherencia.
Conclusión: Existe una asociación significativa entre la adherencia al tratamiento antianémico y
los factores maternos, socioculturales y los relacionados con el tratamiento (p<0.05), sugiriendo que
mejorar la comunicación, el soporte socioeconómico y la accesibilidad podría potenciar la adherencia
terapéutica
Palabras clave: Anemia, adherencia al tratamiento, factores. (Fuente: DeCS
BIREME).
INTRODUCTION
The World Health Organization (WHO) defines anemia in children under 5 years of age as a hemoglobin
concentration <11g/dL at sea level, with iron deficiency being the most common cause
worldwide(1). To
date, a prevalence of up to 39.8% has been calculated, equivalent to 269 million children globally
affected by anemia, making it a significant public health issue(2). In Latin
America, the World Bank
determined in 2019 that the prevalence of anemia was 20%, with Venezuela (28%), Peru (30%), Bolivia
(37%), and Haiti (60%) having the highest rates(3). By 2020, in Peru,
according to Instituto de
Estadística e Informática (National Institute of Statistics and Informatics), 40.1% of children aged 6
to 35 months suffer from anemia, translating to nearly 700 thousand anemic children under 3 years of age
out of 1.6 million nationwide(4). It has been demonstrated that this high
prevalence of anemia in children
can be corrected with iron therapy, and adherence to treatment is essential, meaning the consistent
intake of medication according to prescribed dosages, schedule, and duration.
Additionally, the prevalence is higher in children under 3 years of age due to their rapid growth rate
and consequent iron demands, compounded by low consumption of iron-rich foods, low birth weight,
parasitic infections, and frequent episodes of diarrhea. These factors result in motor development delay
by 10 months, cognitive processing issues by age 10, recognition memory impairment by age 19, and poor
emotional health around age 20(5). According to a 2020 study published in
The Journal of Pediatrics, one
of the primary reasons attributed to the persistent prevalence of childhood anemia is poor adherence to
oral iron therapy(6). The WHO considers this as the degree to which a
patient's behavior regarding
prescribed therapeutic compliance correlates with what is indicated by the healthcare professional,
recognizing it as a severe issue, given that the therapeutic adherence rate for chronic diseases is
approximately 50.0%.(7)
This alarming situation has prompted the Peruvian government to implement iron supplementation for
4-month-old children to prevent anemia, reaching 54.2% coverage in 2021(8).
However, this anemia
prevention plan must evaluate the compliance with such supplementation, as demonstrated by a 2023 study
in the Piura province, where only 47.9% of children completed the treatment(9). It was concluded that more
than 50% of children were not adhering to anemia treatment due to various factors such as residing in
rural areas, micronutrient deficiency in diets, low birth weight, prematurity, maternal anemia, mixed or
artificial breastfeeding, growth rate, iron loss during development, and/or underlying
pathologies(10, 11).
Economic issues, difficulty accessing healthcare facilities, language barriers, beliefs, customs, and
challenges in supplement usage also play significant roles(12, 13).
Regarding factors, they can be defined as "detectable characteristics in individuals associated with a
high likelihood of indicators and may be linked to health."(14) The WHO
classifies adherence-related
factors into four categories: patient-related (economic status, occupation, knowledge, attitudes,
beliefs, fears, perceptions, patient and family expectations, age, parent confidence in healthcare team,
family climate, and positive treatment expectations); therapy-related (complexity and duration of
treatment, previous treatment failures, side effects, and the need for lifestyle changes); healthcare
personnel-related (medication distribution system issues, overburdened healthcare workers, lack of
follow-up interest, lack of support networks, inadequate activity planning, and physician-patient
relationship); and disease-related (physical, psychological, and social risks)(15, 16, 17).
Based on the aforementioned considerations and the high rate of anemia in children under 3 years of age,
this study aimed to determine the factors related to adherence to anti-anemic treatment in children aged
1 to 3 years at the "Señor de los Milagros" Health Center in Huaycán – Ate.
MATERIALS AND METHODS
Study Design and Area
An observational, quantitative, correlational, cross-sectional study was conducted on children aged 1 to
3 years receiving care at the "Señor de los Milagros" Health Center located in Huaycán, district of Ate,
from June 2019 to February 2020.
In 2017, the total population of Ate was 599,196 inhabitants, considered a district of extensive size,
with areas inhabited largely by families of low to middle-low socioeconomic status, as well as families
living in poverty or extreme poverty.
Population and Sample
The study population consisted of 300 mothers with children aged 1 to 3 years undergoing anti-anemic
treatment prescribed at the "Señor de los Milagros" Health Center in Huaycán, Ate. For sample selection,
a simple random probabilistic sampling process was applied using the Epidat 3.4 program, with a
confidence level of 95%, a margin of error of 5%, and a power of 80%. The sample size calculation was
based on the therapeutic adherence variable with an Odds ratio of 3.43, resulting in a sample size of
169 mothers.
Inclusion criteria included surveys with informed consent accepted from mothers with children aged 1 to
3 years attending the "Señor de los Milagros" Health Center diagnosed with anemia and prescribed
anti-anemic treatment between June 2019 and February 2020. Exclusion criteria encompassed surveys from
mothers with children diagnosed outside the specified time frame, those not within the specified age
range, and those who did not provide informed consent to participate.
Variables and Instruments
In the present study, the independent variable considered was the associated factors, which include the
following factors related to the mother: level of education, occupation, and marital status; mother's
sociocultural factor: knowledge about anemia; treatment-related factor: perception of discomfort with
treatment, treatment interruption, improvements observed with treatment, and difficulties with treatment
intake; and health system-related factor: waiting time, doctor-patient interaction, information
provided, and understanding.
On the other hand, the dependent variable was adherence to anti-anemic treatment, which was categorized
as low adherence, medium adherence, high adherence, and non-adherence.
For data collection, a form previously validated and endorsed by 9 subject matter experts was used,
taken from the thesis published in 2010, "Adherence to iron-deficiency anemia treatment in children aged
6 to 24 months and associated factors, C.S.M.I. Tahuantinsuyo Bajo, 2010." The collected data consisted
of 21 questions related to the degree of treatment adherence and associated factors such as mother's
factor, treatment factor, health system factor, and mother's sociocultural factor, with binary response
options (yes, no).
Regarding the levels of adherence, pediatric teaching experts agreed that 12 to 13 affirmative responses
indicated high adherence, 10 to 11 responses indicated medium adherence, 8 to 9 responses indicated low
adherence, and 7 or fewer responses indicated non-adherence.
Procedures
After providing information about the research project and obtaining signed informed consent, the survey
instrument, which was validated and anonymous, was administered to participating mothers. The survey
application time was approximately 20 minutes per participant.
Statistical Analysis
The Statistical Package for the Social Sciences (SPSS) version 23 was used to analyze the data. The
prevalence of the degrees of adherence to anti-anemic treatment and associated factors was described.
Additionally, the association between independent variables and the dependent variable was evaluated
using odds ratios, and population homogeneity was verified using the chi-square test. Data were recorded
in Excel for MacOS 11.0 for the presentation of tables.
Ethical Considerations
The study was authorized by the head of the "Señor de los Milagros" Health Center in Huaycán – Ate, in
accordance with the ethical principles of the Declaration of Helsinki of the World Medical Association
for medical research involving human subjects. Regarding ethical principles, professional conduct will
be maintained by storing patient data without duplication. Confidentiality will be upheld by not
disclosing patient data. Therefore, in accordance with bioethics, justice will be respected in terms of
results, beneficence, and non-maleficence. The information collected from the health center will be kept
confidential, as the data collection form will not request patient names or phone numbers.
- Participation: Participation will be voluntary, with verbal information provided by the interviewer and accepted through prior informed consent.
- Risks: No risks will be posed to the participants.
- Benefits: No personal benefits will be provided, although gratitude will be expressed for the support in raising awareness about the factors associated with adherence to anti-anemic treatment.
- Confidentiality: Survey-generated information will be anonymous, without personal data included for greater reliability.
RESULTS
According to Table 1, the levels of adherence to anti-anemic treatment in children aged 1 to 3 years
show that 55.6% (94) had low adherence, followed by 24.3% (41) with medium adherence, and 4.7% (8) with
high adherence. However, 15.4% (26) had no adherence to the anti-anemic treatment.

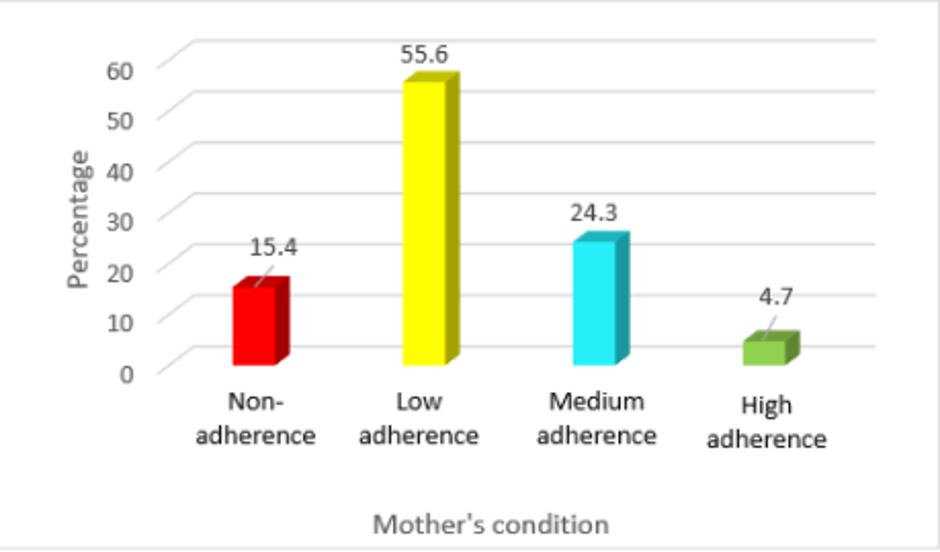
Figure 1. Levels of adherence to anti-anemic treatment in children aged 1 to 3 years at the "Señor de los Milagros" Health Center in Huaycán – Ate.


DISCUSSION
In this study aimed at determining factors associated with adherence to anti-anemic treatment in
children aged 1 to 3 years, it was found that 15.4% of children did not adhere to the prescribed
treatment. These findings are similar to those reported by the World Health Organization (WHO)(2), which
indicates non-adherence rates to any pharmacological treatment ranging from 15% to 93%. However, it is
noted that the adherence observed in our study, although relatively high, predominantly falls within the
medium adherence category, suggesting that mothers meet the minimum requirements prescribed by
healthcare providers.
Adherence to treatment poses a significant public health challenge, necessitating interventions to
eliminate barriers to poor therapeutic adherence to improve population health(9,
15). In a study by Diaz et
al., factors associated with adherence to anti-anemic treatment in children under 3 years were related
to the absence of the caregiver (58%) and lack of attendance at health services (44%)(18). Moreover,
adherence to treatment becomes more challenging and complex when the treatment duration is long with
daily dosing, requiring effort, time, and knowledge about the treatment by the mother or
caregiver(8, 16).
The current study demonstrated that various maternal factors, such as secondary education attainment,
occupation as a homemaker, and cohabiting marital status, exhibited a higher level of medium and low
adherence (p<0.05). Additionally, maternal education and closeness to the child contribute to better
anemia treatment(10, 16). When considering sociocultural
and treatment-related factors associated with
adherence to anti-anemic treatment (Table 3), it was found that all of them acknowledge anemia as a
serious condition, with meat and legumes being the richest sources of iron. Only 55 mothers believed
that anemia can be cured solely with iron, followed by the majority (157 mothers) advocating for
iron-rich dietary intake alone, and 152 mothers indicating that treatment is prolonged. On the other
hand, concerning treatment-related factors, side effects such as constipation and dark stool color were
reported, leading 52% of mothers to discontinue treatment. Nevertheless, 94% of mothers believed that
their child was improving with treatment, with 90% of them administering iron without difficulty,
although 55% found it challenging to prepare iron-rich foods daily. Other studies have reported similar
findings(10). All these associations correspond to low adherence.
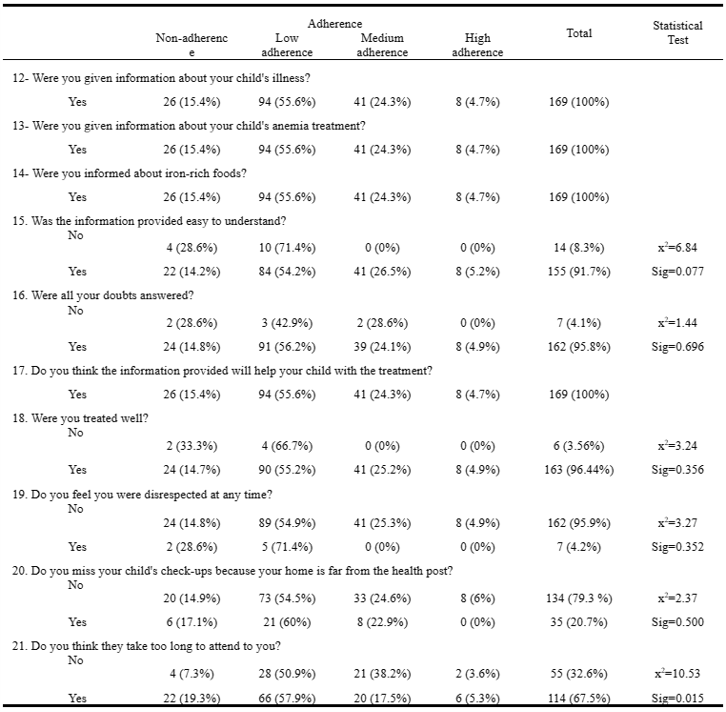
Among the factors of the health system associated with adherence to anti-anemic treatment (Table 4), we
observed that regarding the information provided to the mother, there is adherence to knowledge of the
child's disease, treatment of anemia, the information was easily understandable, all doubts were
answered including which foods are rich in iron, and she is confident that all this information will aid
in her child's recovery process. Adherence to all these information factors was mostly of low category.
On the other hand, the treatment received by the mothers was good, there was no disrespect at any time,
the mother does not miss her child's appointments despite the distance, and if she feels they take too
long to attend to her (all adherence ranging from low to medium), the p value is less than 0.05. Several
studies have had similar findings(13, 14, 18). To improve adherence, strategies such as simplifying
treatment regimens, counseling sessions, reminder systems, supervision and incentives for healthcare
personnel, family therapy, psychological therapy, and phone follow-up(19)
are recommended. Currently,
there is a willingness to combine more than one strategy to reinforce the message and increase impact.
For our case of anemia, options would include communicative educational intervention, family and
community involvement, and strengthening monitoring, supervision, and surveillance systems(17, 18). We
consider that in this study, some values found have discrepancies in terms of their level of
significance; therefore, it is necessary to conduct further analytical studies with more representative
samples to identify factors according to each context.
CONCLUSIONS
- A total of 15.4% of mothers did not fully adhere to the prescribed treatment.
- Mothers with secondary education and homemakers showed the highest levels of adherence (low to medium).
- Regarding maternal knowledge about anemia, higher adherence was observed among mothers who:
- Recognized anemia as a serious condition.
- Understood the importance of prolonged treatment and iron-rich foods.
- Perceived improvement in their child's health with treatment.
- Factors associated with higher adherence included:
- Receiving information that was easy to understand.
- Experiencing respectful treatment without disrespect.
- Facing challenges in attending their child's appointments due to the distance from their residence.
Authorship contributions:
ILOH participated in conceptualization, research, methodology, resourcing, and drafting of
the original manuscript. LEPG participated in conceptualization, methodology, and original
draft supervision.
Financing:
Self-funded
Declaration of conflict of interest:
The authors declare no conflict of interest.
Recevied:
January 24, 2024
Approved:
April 11, 2024
Correspondence author:
Imelda Lourdes Oscanoa Huamán
Address:
Calle Guadalupe 555. Condominio Depa + Club Huachipa, Ate, Lima-Perú.
Phone:
(+51) 986099174 - 993618741
E-mail:
imilourdes@hotmail.com
Article published by the Journal of the faculty of Human Medicine of the Ricardo Palma University. It is an open access article, distributed under the terms of the Creatvie Commons license: Creative Commons Attribution 4.0 International, CC BY 4.0 (https://creativecommons.org/licenses/by/1.0/), that allows non-commercial use, distribution and reproduction in any medium, provided that the original work is duly cited. For commercial use, please contact revista.medicina@urp.edu.pe.
BIBLIOGRAPHIC REFERENCES
