

EDITORIAL
DOI 10.25176/RFMH.v19.n1.1788ASSOCIATION BETWEEN AGE AND TYPE OF LESION FOUND BY LOWER GI ENDOSCOPY IN PATIENTS WITH LOWER GI BLEEDING, SANTA ROSA HOSPITAL-2015
ASOCIACIÓN ENTRE LA EDAD Y TIPO DE LESIÓN ENCONTRADA POR ENDOSCOPIA BAJA EN PACIENTES CON HEMORRAGIA DIGESTIVA BAJA, HOSPITAL SANTA ROSA-2015
María Elena Sandoval-Pereda1,a,Jorge Burgos-Miranda2,b,c
1Hospital Santa Rosa, Lima-Perú.
2Hospital Daniel Alcides Carrión, Lima- Perú.
aInterno de Medicina
bMédico Cirujano
cEspecialista en Cirugía Plástica.
ABSTRACT:
Objective:
To determine the association between age with the types of lesions found in
patients diagnosed with low digestive bleeding undergoing low endoscopy in the Gastroenterology service of
Santa Rosa Hospital.
Methods:
Observational, analytical, retrospective study, information was collected
from the reports of low digestive endoscopy and medical history files of the Gastroenterology service.
Variables: age, sex, type of injury and anatomical location of the lesion; it was summarized to cards for
their statistical use using the SSPS version 22 and Excel programs for the graphs and tables, Chi square
test was used, with a value of p less than 0.05 as statistically significant.
Results:
Sample of 180 patients
with an
average age of 62 years, divided into G1: (18-34 years) with 10% of the sample, the endoscopic examination
predominates without evidence of injury, followed by hemorrhoids, G2: (35-64 years) with 38% of the sample,
external hemorrhoids predominate, G3: (65 to more) with 52% of the sample, internal hemorrhoids
predominate, with respect to sex 60% are female; The most frequent anatomic location was found at the level
of the rectum-anus. In addition, the association between patients less than 35 years and 35 years old more
than the
presence or absence of endoscopic lesion, generated an OR 18,514 which was statistically significant.
Conclusion:
It is concluded that there is an association between age and / or age group with the type of
endoscopic lesion found, predominantly the age group GIII corresponding to adults over 65 years of age, in
which the highest number of internal hemorrhoids was found. and external; there being an association
between the age of the patient with the presence of endoscopic lesion, with an OR of 18.5; this indicates
that there is an 18.5 times higher risk than an older patient with lower gastrointestinal bleeding found by
low endoscopy, which is why this relationship was statistically significant.
Key words:
Lower gastrointestinal bleeding; Anatomical location of the lesion; Type of endoscopic lesion (source: MeSH NLM)
RESUMEN:
Objetivo:
Determinar la asociación entre la edad con los tipos de lesiones encontradas en pacientes
con diagnóstico de hemorragia digestiva baja sometidas a endoscopia baja en el servicio de Gastroenterología
del hospital Santa Rosa.
Métodos:
Estudio observacional, analítico, retrospectivo, se recopiló información
proveniente de los informes de endoscopia digestiva baja y los archivos de historia clínica del servicio de
Gastroenterología del Hospital Santa Rosa. Se tuvo en cuenta las siguientes variables: edad, sexo, tipo de
lesión y localización anatómica de la lesión; se resumieron a fichas para su uso estadístico utilizando los
programas de SSPS versión 22 y Excel para los gráficos y tablas, se usó la prueba de Chi cuadrado, con un
valor de p menor a 0,05 como estadísticamente significativo para obtener los resultados necesarios para la
investigación.
Resultados
Teniendo una muestra significativa de 180 pacientes con una edad promedio de
62
años, divididos en G1: (18-34 años) con un 10% de la muestra, predomina el examen endoscópico sin evidencia
de lesión, seguido de hemorroides, G2: (35-64 años) con un 38% de la muestra, predomina hemorroides
externas, G3: (65 a más) con un 52% de la muestra, predomina hemorroides internas, con respecto al sexo 60%
son de sexo femenino; la localización anatómica más frecuente se encontró a nivel del recto-ano. Además la
asociación entre pacientes menor a 35 años y 35 años a más respecto a la presencia o no de lesión
endoscópica, nos
generó un OR de 18.514 el cual fue estadísticamente significativo, con lo que concluimos que tener más de
35 años incrementa en 18.5 veces el riesgo de presentar una lesión endoscópica y según la prueba de Chi
cuadrado, se concluye que si existe relación significativa entre la edad y la presencia de lesión
endoscópica.
Conclusión:
Se concluye que existe asociación entre la edad y/o el grupo etario con el
tipo de
lesión endoscópica encontrada, predominando el grupo etario GIII que corresponde a los adultos mayores de
65 años, en el que se encontró la mayor cantidad de hemorroides internas y externas; habiendo asociación
entre la edad del paciente con la presencia de lesión endoscópica, con un OR de 18.5; lo cual nos indica
que existe 18.5 veces más riesgo que un paciente a mayor edad presente hemorragia digestiva baja encontrada
por endoscopia baja, por lo cual esta relación fue estadísticamente significativa.
Palabras clave:
Hemorragia digestiva baja; Localización anatómica de la lesión; Tipo de lesión endoscópica. (fuente: DeCS
BIREME)
INTRODUCTION
In Peru, 10-15% of all gastrointestinal bleeding present by total population correspond to a lower gastrointestinal bleeding (LGIB); however, numbers are higher (20-30%) in elderly. In addition, hospitalization rate due to LGIB dramatically increases 200 times more after 80 years old1.
The highest LGIB incidence in elderly is related to an increase in prevalence of diverticular disease of the colon and angiodysplasia with aging. It is difficult to search the origin of LGIB in some cases, due to the vast region composed by small and large intestine2.
Many studies have concluded that age influences the presence or absence of lower GI bleeding, since the older the person, the most frequent it is to find cases of lower GI bleeding worldwide3-6.
It is to be considered that lower GI bleeding self-limits in 85% of cases, whereas in the 15% left, it remains active. These last cases need a prompt attention given that almost 50% of cases require emergency surgical treatment7.
Nowadays, annual incidence of patients who present severe LGIB goes from 20.5 to 27 cases/100 000 inhabitants and its global mortality is less than 5% of the total. It mostly predominates in male sex, it also generally appears in elderly, mainly 75 years old to more and it is usually associated with serious illness or even with history of surgical operations8-10.
Lower gastrointestinal bleeding represents itself a serious health problem for current community. It does not only constitutes a serious problem in terms of morbi-mortality, but also a budget problem for a health system who struggles to stand up year after year due to great demand of health services for this reason11.
Inside the universe of lower gastrointestinal bleedings, there are numerous etiologies. Even though most of them are self-limited or mild problems typical of the age such as inflammation and diverticulosis, there are also poor prognosis etiologies such as colon cancer, which represents much suffering and ailment both physical and psychological for the correspondent patient, as well as a great expense in medicines and procedures financed mostly by the state12.
In this work, we search to know better about LGIB, as well as types of lesions related to diverse pathologies of which LGIB only represent an important clinical sign. All this from a statistical point of view based in evidence found in colonoscopies supported by specialists in the field. We will see to which etiology / illness it takes us, so that we can have a clinical suspicion related to age, sex, with a scientific basis of evidences of a whole year.
We have chosen the year 2015 due to its proximity.
Thus, in this research we seek to know the association between age and type of lesion found in patients diagnosed with lower gastrointestinal bleeding undergoing lower gastrointestinal endoscopy in the gastroenterology service of Santa Rosa hospital during the year 2015.
METHODS
We carried out an observational, analytical and retrospective study, which collected information from the reports of lower gastrointestinal endoscopy and medical history files of the gastroenterology service of Santa Rosa. We considered the following variables: age, sex, type of lesion and anatomical location of the lesion. They were summarized to cards for their statistical use using the SSPS version 22 and Excel programs, which determined the relationship in the graphs and tables, using the Chi square test, with a value of p<0.05 as statistically significant in order to achieve the necessary results for the research.
The execution of this work started with the presentation and corrections of this work to the authorities of the Biomedical Sciences Research Institute (INICIB, for its acronym in Spanish) from the Faculty of Human Medicine of the Ricardo Palma University, and wait until its approval. Then, we requested the hospital administrator the permissions and facilities to access the clinical records and reports of lower gastrointestinal endoscopy, from January 2015 to December 2015. Once we have the permission, we proceeded with coordination with archives staff and we carried out the data collection through collection of information from clinical records and reports of lower gastrointestinal endoscopy from the general medical service of Santa Rosa hospital during the year 2015, which were transcribed to a data collection card for use.
Once we obtained data through clinical records and reports of lower gastrointestinal endoscopy, we tabulated them and presented them in graphs and tables selected for that purpose. We applied Chi square statistical test to carry out sample analysis, with a p<0.05 as significant and a confidence interval of 95%.
RESULTS
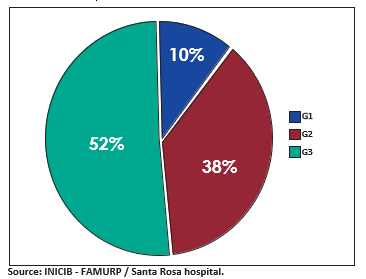
Graph 1. Division by age group
Graph 1 shows that from a significant sample of 180 patients, median age was 62 years old. It was divided in G1 (18- 34 years old), G2 (35-64 years old) and G3 (65 years old to more) which represent the 10%, 38% and 52% of the sample, respectively.
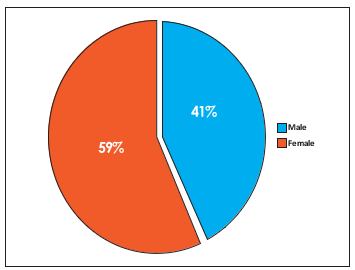
Graph 2. Division by sex.
In graph 2, we found a partial prevalence of female sex that represents 60% of the sample, versus 40% of male sex.
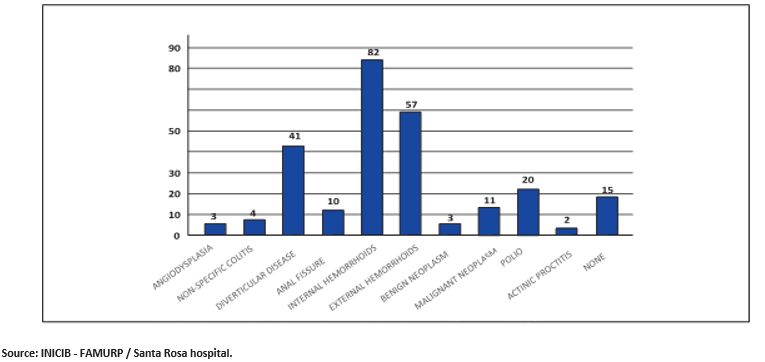
Graph 3. Type of endoscopic lesion in LGIB
We observe in graph 3 that the most prevalent lesion was internal hemorrhoids, diagnosed in 82 patients that represents 45.55% of patients affected by this disease, followed by external hemorrhoids in 57 patients (31.66%). The least prevalent was actinic proctitis in 2 cases (1.11%). No injury was found in 15 cases representing 8.33% of patients.
Table 1.Patients with diagnosis of lower gastrointestinal bleeding, with and without lesion found by lower gastrointestinal endoscopy, Santa Rosa hospital, 2015.
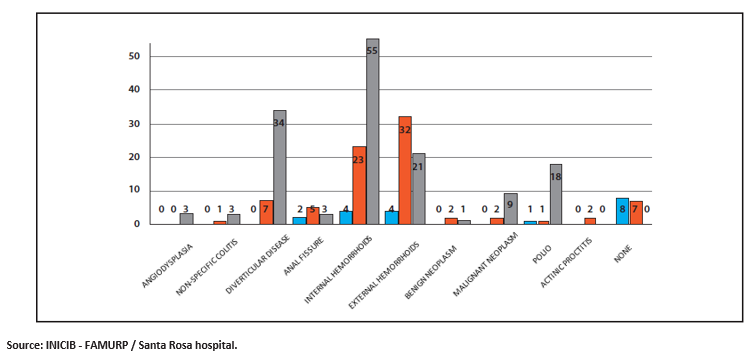
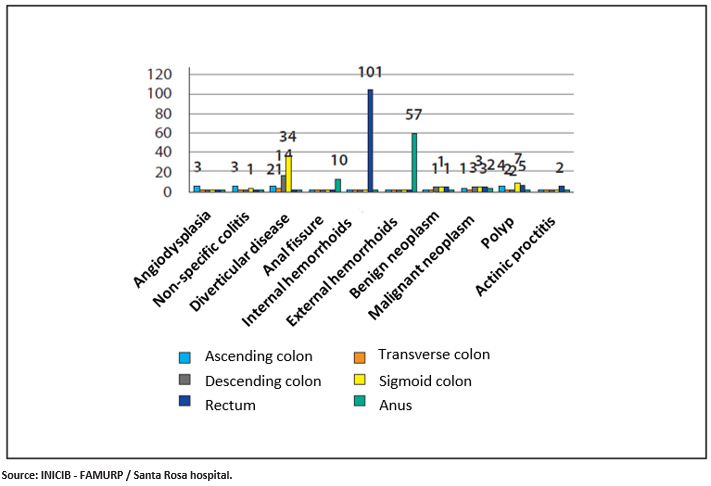
Graph 4. Type of lesion by age group
In graph 4, regarding age group G3, it predominates internal hemorrhoids (55 cases), diverticular disease (34 cases) and external hemorrhoids (21 cases). Regarding G2, it predominates external hemorrhoids (32 cases). Regarding G1, it predominates examination without evidence of endoscopic lesion.
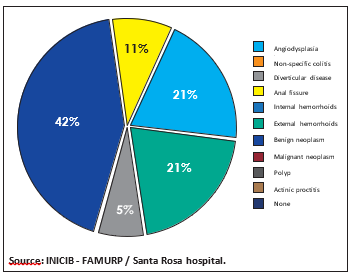
Graph 5. Type of lesion in age group I (18-34 years old).
In this graph 5, we observe that there was no lesion evidenced in 42% of the patients. In 21%, we found internal and external hemorrhoids. In lower percentages, anal fissure and polyps.
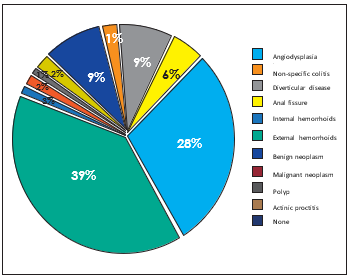
Graph 6. Type of lesion in age group II (35-64 years old).
In graph 6, we obtained a 39% of patients with external hemorrhoids, followed by a 28% of patients with internal hemorrhoids. In a lower percentage, we obtained benign and malignant neoplasm with 9% each one, anal fissure with 6%, whereas the other diseases in percentages under 3%.
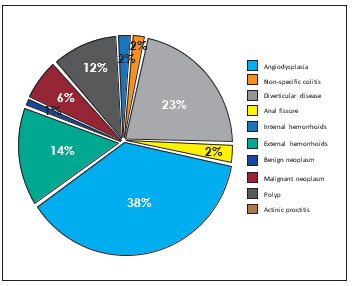
Graph 7. Type of lesion in age group III (65 years old to more).
Regarding age group III (graph 7), we obtained 38% of patients with internal hemorrhoids, followed by 23% of patients with diverticular disease, 14% with external hemorrhoids and 12% with polyps, in a lower percentage we obtained malignant neoplasm with 6%, whereas the other diseases in percentages under 3%.
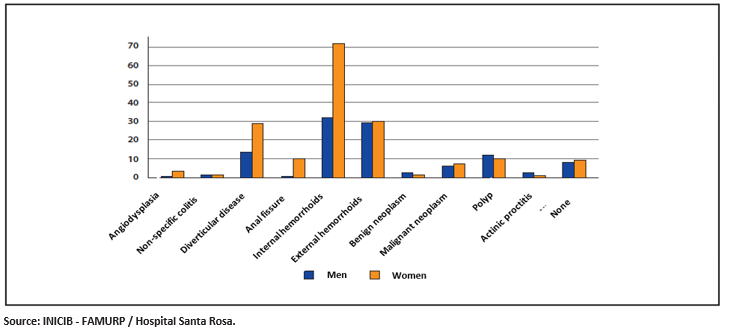
Graph 8. Type of lesion according to gender.
In graph 8, we found prevalence of internal hemorrhoids in female sex, in a relationship of nearly 2:1, whereas in external hemorrhoids the numbers are similar for both male and female. Regarding diverticular disease, we found prevalence in female sex of 2:1, as well as in anal fissure where female sex prevails with 9:1, whereas in angiodysplasia the total corresponds to female sex. Regarding male sex, we found a prevalence of polyps in a relationship of 11:9.
Graph 9. Most frequent anatomical location of the type of lesion.
Finally, in graph 9 we obtained a prevalence of internal hemorrhoids in the rectum with a 100% of cases, external hemorrhoids in the anus with a 100% of cases, diverticular disease predominated in sigmoid colon (82.92%), anal fissure (100%) in the anus. Polyps predominated in sigmoid colon (35%), angiodysplasia in ascending colon with a 100% of cases, non-specific colitis in ascending colon (75%), malignant neoplasm predominated in descending colon, sigmoid colon and rectum (25% each one), actinic proctitis in the rectum with a 100% of cases.
DISCUSSION
Lower gastrointestinal bleeding represents a serious health problem for current society since it has a high morbidity rate, thus, we have to know both the causes and the most proper treatment for this health problem. In Santa Rosa hospital, we obtained 342 endoscopic reports of patients diagnosed with lower gastrointestinal bleeding. Average age in the population was 62 years old, where the most prevalent age group was G3 (65 years old to more), representing more than half the study population (52%). These results agree with most of the studies quoted in this work.
Afterwards, we carried out age assessment as a condition related to the presence or absence of endoscopic lesion, observing the distribution of patients depending on the contingency table. Then, we calculated the respective statistical parameters beginning with odds ratio whose value turned out to be 18.5. This value expresses the following: patients who are 35 years old to more are related to presence of endoscopic lesion, corresponding to 18.5 times more than those patients under 35 years old.
Thus, statistical analysis through chi square test performs the function of determining statistical significance of obtained distribution, in this particular case the found significance turns out to be positive. This implies that the possibility of the influence of chance in association described between both variables is under 5%, which proves to be the least expected. The results have a proper strength of association because its value is greater than 2, thus in the conclusion, the association between both variables turns out to be decisive.
Regarding sex, we registered partial prevalence in female sex that represents a 59% (106 patients) compared with a 41% of male sex (74 patients). This result shares similarity with two other studies. Geraud Elisa, Ríos Isabel and Francis Pedro carried out the first study, in Hospital General del Oeste, in Caracas, where the study population was 389 patients, of which 55.7% were women and 44.3% were men13. Javier Jesús Suárez Rivera from Hospital Clínico Quirúrgico “Julio Trigo” in La Habana carried out the second study. This one mentions the difference between men and women, in this case female sex predominated (8 versus 714, unlike what most of the bibliography indicates.
In addition, we found in our study the prevalence of internal hemorrhoids in female sex in a relationship of nearly 2:1, whereas in external hemorrhoids the numbers are similar for both male and female. Regarding diverticular disease, we found prevalence in female sex of 2:1, as well as in anal fissure where female sex prevails with 9:1, whereas in angiodysplasia the total corresponds to female sex. Regarding male sex, we found a prevalence of polyps in a relationship of 11:9.
The most frequent endoscopic lesions found in lower gastrointestinal endoscopy reports during the year 2015 were internal hemorrhoids with a percentage of 45.55% of patients, followed by external hemorrhoids with a percentage of 31.66% of patients, diverticular disease with 22.77%, polyps with 11.11%, malignant neoplasm with 6.11%. Two studies present similar results. Cristian Mendez Cordova, Pedro Barrós, José Cabello and Alejandro Bussalleu carried out the first study in Cayetano Heredia National Hospital, in Lima. Geraud Elisa, Ríos Isabel and Francis Pedro carried out the second study, in Hospital General del Oeste, in Caracas13. In both of them, the diagnosis of hemorrhoids, diverticula and polyps headed the incidence of type of lesion found.
Concerning age groups, we found that in age group I (18-34 years old) the absence of endoscopic lesion predominated, followed by hemorrhoids, as in the study carried out by José Alberto Marín A. in Mexico, where we could find similar results. In age group II (35-64 years old), we found prevalence of hemorrhoids with a 67%, and in a lower percentage we obtained benign and malignant neoplasm with 9% each one, as in José Alberto Marín A.’s study. In age group III (65 years old to more), we found prevalence of hemorrhoids with a 52%, followed by a 23% with diverticular disease, a 12% with polyps. We obtained malignant neoplasm in a lower percentage with 6%. Besides, the cases of angiodysplasia and non-specific colitis belong almost entirely to this age group. These data was similar to José Alberto Marín’s study.
In terms of anatomical location of lesion, we found a prevalence of internal hemorrhoids in the rectum with a 100% of cases, external hemorrhoids in the anus with a 100% of cases, diverticular disease in sigmoid colon (82.92%) and descending colon (34.14%). Anal fissure (100%) in the anus. Polyps in sigmoid colon (35%), rectum (25%), ascending colon (20%), transverse colon (10%) and descending colon (10%). Angiodysplasia in ascending colon with a 100% of cases. Non-specific colitis in ascending colon (75%) and sigmoid colon (25%). Malignant neoplasm in ascending colon (8.33%), descending colon (25%), sigmoid colon (25%), rectum (25%) and anus (16.66%). Actinic proctitis in the rectum with a 100% of cases. These data is similar to those referred in the theoretical texts.
CONCLUSION
Based on the obtained results, we conclude that it exists association between age and/or age group and type of endoscopic lesion found. Age group GIII (65 years old to more) predominated. In this group, we found the largest number of internal and external hemorrhoids. Besides, diverticular disease, polyps and malignant neoplasm in a lower percentage, which agrees with theory correspondent to age versus type of lesion. We found association between age of patient and presence or absence of endoscopic lesion, with an OR of 18.5, which indicates us that there is a 18.5 more times risk that an elderly patient presents lower gastrointestinal bleeding found by lower gastrointestinal endoscopy, thus, this association was statistically significant. In addition, we found that female sex presents internal hemorrhoids more frequently, whereas regarding external hemorrhoids the numbers are similar for both male and female. Regarding diverticular disease, we found prevalence in female sex of 2:1, as well as in anal fissure where female sex prevails with 9:1, whereas in angiodysplasia the total corresponds to female sex. Concerning neoplasms, we found similarities in both male and female sex. In contrast, regarding male sex, we found a prevalence of polyps in a relationship of 11:9. In addition, we found a prevalence of internal and external hemorrhoids in a 100% of cases in the rectum and the anus, respectively. Diverticular disease predominated in sigmoid colon with 82.9%. Polyps in sigmoid colon with 35%. Angiodysplasia in ascending colon with a 100% of cases. Non-specific colitis in ascending colon with 75%. Malignant neoplasm in descending colon, sigmoid colon and rectum, with 25% each one. Actinic proctitis in the rectum with a 100% of cases. These data corresponds to patients from gastroenterology service of Santa Rosa hospital during the year 2015.
Authorship contribution: The author participated in the creation, writing and final approval of the original article, as well as in data collection.
Financing: Self-financed.
Conflict of interest: The author declares that she has no conflict of interest with the publication of this article.
Received: September 26th, 2018
Approved: December 19th, 2018
Correspondence: María Elena Sandoval Pereda
Address: Avenue República de Panamá 350-Dpto 401, Lima-Perú
Telephone: +51993726650
Email: marielena-17-89@hotmail.com
BIBLIOGRAPHICAL REFERENCES
-
1. Rubio P, Ortiz Hurtado H, Velasco M. Función defecatoria y calidad de vida con la cirugía preservadora de
esfínteres en el cáncer de recto. Cirugía española: Organo oficial de la Asociación Española de Cirujanos
2003,Vol. 73, Nº. 1:52-57.
2. Miño G, Soriano A, González A, Hervás A J, Naranjo A. Hemorragia digestiva baja grave. Rev And Patol Digest1997: 20: 128-132.
3. Vázquez Sequeiros E, Albillos Martínez A. Protocolo diagnósticoterapéutico de hemorragia digestiva baja. Medicine: Enfermedades del aparato digestivo. Patología intestinal y del peritoneo Medicine: Enfermedades del aparato digestivo. Patología intestinal y del peritoneo 2004, Serie 9, Nº. 5: 369-372
4. Zuckerman GR, Prakash C, Askin MP, Lewis BS. AGA Technical review on the evaluation and management of occult and obscure gastrointestinal bleeding. Gastroenterol 2000;118(1):201-221.
5. Church J. Adenoma Detection Rate and the Quality of Colonoscopy: The Sword has Two Edges. Dis Colon Rectum 2008; 51: 520-523.
6. Kovacs TOG, Jensen DM. Endoscopic control of gastroduodenal hemorrhage. Ann Rev Med 1987;38:267- 277.
7. Junquera F, Quiroga S, Saperas E. Et al. Accuracy of helical computed tomographic angiography for the diagnosis of colonic angiodysplasia. Gastroenterology 2000; 119(2):293-299.
8. Chol YB, Lim KS. Therapeutic laparoscopy for abdominal trauma.Surg Endosc. 2003;17(3):421-7
9. J.J. Farrell,L.S. Friedman Review article: the management of lower gastrointestinal bleeding Aliment Pharmacol Ther, 21 (2005), pp. 12811298
10. R.E. Davila,E. Rajan,D.G. Adler,J. Egan,W.K. Hirota,J.A. Leighton ASGE Guideline: the role of endoscopy in the patient with lower-GI bleeding Gastrointest Endosc, 62 (2005), pp. 656-660
11. F. Rodriguez Moranta,A. Berrozpe,J. Guardiola Diagnostic performance of colonoscopy in lower gastrointestinal bleeding Gastroenterol Hepatol, 34 (2011), pp. 551-557
12. L.L. Strate,C.R. Naumann The role of colonoscopy and radiological procedures in the management of acute lower intestinal bleeding. Clin Gastroenterol Hepatol, 8 (2010), pp. 333-343
13. Geraud Elisa, Ríos Isabel, Francis Pedro, Ollarves María, Gori María, Folkmanas William et al. Hallazgos endoscopicos en pacientes con hemorragia digestiva inferior en el Hospital General del Oeste durante los años 2003-2008. Gen [Internet]. 2010 Sep [citado 2018 Mar 2] ; 64( 3 ): 180-185. Disponible en: http://www.scielo.org.ve/scielo.php?script=sci_arttext&pid=S0016-35032010000300007&lng=es
14. Suárez J. Caracterización-de-pacientes fallecidos-por-hemorragiadigestiva-baja. Revista portales médicos.com [Internet]. 2014 Feb. [citado 2018 Feb Disponible en: https://www.revista-portalesmedicos.com/revista-medica/publicaciones/gastroenterologia/caracterizacion-depacientes-fallecidos-por-hemorragia-digestiva-baja/
15. Geraud Elisa, Ríos Isabel y Francis Pedro en el Hospital General del Oeste en Caracas
16. Javier Jesús Suárez Rivera del Hospital Clínico Quirúrgico “Julio Trigo” de La Habana
17. Cristian Méndez Córdova, Pedro Barrós,José Cabello, Alejandro Bussalleu en el Hospital Nacional Cayetano Heredia 18. José Alberto Marín A. en México
