ORIGINAL ARTICLE
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2019 - Universidad Ricardo PalmaDOI 10.25176/RFMH.v19i4.2342
CLINICAL EPIDEMIOLOGICAL CHARACTERISTICS OF PARKINSON'S DISEASE IN A NATIONAL HOSPITAL OF THE PERUVIAN HIGHLANDS
CARACTERÍSTICAS CLÍNICO EPIDEMIOLÓGICAS DE LA ENFERMEDAD DE PARKINSON EN UN HOSPITAL NACIONAL DE LA SIERRA PERUANA
Iván R. Condor1,a, Joel I. Atencio-Paulino1,b, Coco R. Contreras-Cordova1,c
1 Faculty of Human Medicine, National University del Centro del Perú-Huancayo
a Surgeon
b Medical student
c Geriatrician
ABSTRACT:
Objective: To determine the main epidemiological and clinical characteristics of Parkinson's disease at the National Hospital "Ramiro Prialé Priale" in EsSalud-Huancayo. Methods: Observational, descriptive retrospective study of a series of cases. 84 patients were studied between 2015 and 2017, treated in the outpatient clinic or hospitalization of Neurology and Internal Medicine, for which their medical records were reviewed, the sampling was non-probabilistic of the census type selected by the investigator's judgment. Results: The average age was 72.93 years, the male gender prevailed (58.3%), the degree of university education (50%) and the origin of Huancayo (77.4%). Decompensated arterial hypertension was the reason for hospitalization (19.1%), disease time ranged from 1-7 years (57.1%) and tremor at rest and bradykinesia was the most frequent motor symptom (23, 8%) In non-motor symptoms, 38.1% had sleep disorders, 21.4% family history of Parkinson's disease and the most associated comorbidities were: depression (48.8%) and insomnia (41.7%). Conclusion: Parkinson's disease is a frequent pathology in older adults and in the male sex; The predominant motor symptom is resting tremor and bradykinesia, and the associated neuropsychiatric comorbidities are depression and insomnia.
Keywords: Parkinson's disease; Hypokinesia; Disorders of onset and maintenance of sleep. (Source: DeCS BIREME)
RESUMEN
Objetivo: Determinar las principales características epidemiológicas y clínicas de la enfermedad de Parkinson en el Hospital Nacional “Ramiro Prialé Priale” de EsSalud-Huancayo Métodos: Estudio observacional, descriptivo tipo retrospectivo de una serie de casos. Se estudió 84 pacientes entre los años 2015 y 2017, atendidos en la consulta externa u hospitalización de Neurología y Medicina interna, para ello se revisó sus historias clínicas, el muestreo fue no probabilístico de tipo censal seleccionados por juicio del investigador. Resultados: El promedio de edad fue 72,93 años, predominó el género masculino (58,3%), el grado de instrucción universitario (50%) y la procedencia de Huancayo (77,4%). La hipertensión arterial descompensada fue el motivo de hospitalización (19,1%), el tiempo de enfermedad tuvo un rango de 1-7 años (57,1%) y el temblor de reposo y bradicinesia fue el síntoma motor más frecuente (23,8%). En los síntomas no motores, 38,1% tuvieron alteraciones del sueño, 21,4% antecedentes familiares de enfermedad de Parkinson y las comorbilidades más asociadas fueron: depresión (48,8%) e insomnio (41,7%). Conclusión: La enfermedad de Parkinson es una patología frecuente en adultos mayores y en el sexo masculino; el síntoma motor que predomina es el temblor de reposo y bradicinesia, y las comorbilidades neuropsiquiátricas asociadas son la depresión e insomnio.
Palabras Clave: Enfermedad de Parkinson; Hipocinesia; Trastornos del inicio y del mantenimiento del sueño. (Fuente: DeCS BIREME)
According to WHO, the condition of Parkinson's disease was one person for every 100 people over 60 years in 2016, being in absolute figures 6.3 million people, and by 2030 there will be approximately 12 million people worldwide with this pathology1. In 2008, PAHO identified that patients with epilepsy, Parkinson's disease, and Alzheimer's disease together accounted for more than 6% of the global burden to medical institutions2. Parkinson's disease in the United States affects approximately more than one million people, the vast majority of whom are over 50 years3.
In Peru, there are no official or exact figures, the National Institute of Neurological Sciences (INCN) estimated in 2014 that 1% of the population in general had Parkinson's disease, or approximately 300,000 people4. In Peru, it is estimated that by 2030 there will be 2,015,065 people with Parkinson's disease and a mortality rate of 25.45 per 100,000 people5. Every year between 2,000 and 3,000 new cases are reported in our country, and in the city of Lima there are approximately 10,000 people with this disease6.
The social health insurance EsSalud tries to provide a more comprehensive care, from rehabilitation therapies to additional drugs in case of comorbidities and surgery for stimulation in severe cases (applied since 2007)7.
A study was carried out on the prevalence of this disease, with the Junin region being the second place in terms of birth and origin after Lima Metropolitan area, and its relationship with toxins was also determined, especially with the use of some pesticides8. The objective of this research is to determine the main characteristics (clinics, epidemiological, treatment and comorbidities) of Parkinson's disease.
METHODS
Type and design
This is a retrospective observational study that analyzed a series of clinical cases. The place of execution was the Ramiro Prialé Prialé hospital of Huancayo.
Population and sample
Patients who met the criteria for Parkinson's disease, treated in the outpatient clinics and/or in the inpatient room of the neurology and/or internal medicine services, between July 2015 and July 2017, at the Ramiro Prialé Prialé hospital.
It was decided to study the entire available population, in this case of census type, which was approximately 120 patients that after the selection with the criteria proposed by the researchers remained 84. In addition, the sampling was non-probabilistic and was based on the criteria or judgment of the researchers9,10; We included the medical records of patients diagnosed with Parkinson's disease who were hospitalized in the internal medicine service and/or treated in the external neurology offices of the National Hospital "Ramiro Prialé Prialé" of Huancayo during the years 2015 and 2017, ruling out the clinical records have incomplete records.
Methods of analysis and data collection
A form was developed for each patient with Parkinson's disease, containing the parameters: epidemiological, clinical and comorbidity, validated by expert judgment, this validation by criterion or content by teachers of the Faculty of Human Medicine – UNCP, also a pilot test was done to see the reliability of the data collection form resulting in good reliability with a Cronbach's alpha 0.81.
Statistical analysis
First, descriptive statistics were used for quantitative data, central tendency and dispersion measures were used, so for qualitative or categorical variables frequencies and percentages, as well as the use of graphs such as the bar diagram. Statistical programs such as SPSS 24.0, Epi Info 4.0, Med Clac and Excel 2016 were used for the analysis. The collection and analysis was carried out by the authors who participated in this research.
Ethical considerations
The following research work was carried out with the authorization of the institution with the assurance that the data obtained will be used only for scientific purposes, preserving the anonymity of all patients, as well as the ethical guidelines for research promoted by the National Hospital "Ramiro Prialé Prialé" of Huancayo.
RESULTS
84 medical records that met the criteria for selection of researchers were reviewed, in Table 1, you can see the epidemiological characteristics, the average age was 72.93 years with a IC of 95%: (54.71- 91.15), with a standard deviation of 9.298 being the minimum 50 and maximum 90 years; Regarding gender, males were more frequent (58.3%), also married marital status predominated (69%), the degree of university education (50%) and Huancayo as place of origin (77.4%).
Table 1. Epidemiological characteristics of patients with Parkinson's disease at the Ramiro Prialé Prialé Hospital of Huancayo.
| Media |
IC 95% | |
| Age (n=84) | 72,93±9,30 | 54,71 - 91,15 |
| Gender (n=84) | (n) | (%) |
| Male | 49 | 58,3 |
| Female | 35 | 41,7 |
| Marital Status (n=84) | (n) | (%) |
| Married | 58 | 69,0 |
| Single | 19 | 22,6 |
| Widower | 6 | 7,1 |
| Divorced | 1 | 1,2 |
| Level of instruction (n=84) | (n) | (%) |
| No education | 3 | 3,6 |
| Primary education | 5 | 6,0 |
| Secondary education | 23 | 27,4 |
| Non-university higher education | 11 | 13,1 |
| University degree | 42 | 50,0 |
| Origin (n=84) | (n) | (%) |
| Huancayo | 65 | 77,4 |
| Jauja | 5 | 6,0 |
| Concepción | 3 | 3,6 |
| Tarma | 3 | 3,6 |
| Yauli | 1 | 1,2 |
| Junín | 1 | 1,2 |
| Others | 6 | 7,1 |
Table 2. Clinical characteristics of patients with Parkinson's disease from the Ramiro Prialé Prialé Hospital of Huancayo.
| Reason for hospitalization (n=41) | (n) | (%) |
| Decompensated arterial hypertension | 16 | 19,1 |
| Chronic cholecystitis | 10 | 11,9 |
| Clavicle trauma | 4 | 4,8 |
| Olecranon trauma | 3 | 3,6 |
| Ventral hernia | 2 | 2,4 |
| Hip trauma | 2 | 2,4 |
| Pelvic trauma | 2 | 2,4 |
| Varicose veins | 2 | 2,4 |
| Disease time (n=84) | (n) | (%) |
| Between 1 - 7 years | 48 | 57,1 |
| Between 8 – 14 years | 24 | 28,6 |
| Over 14 years | 9 | 10,7 |
| Under 1 years | 3 | 3,6 |
| Disease time (n=78) | (n) | (%) |
| Tremor and bradykinesia | 20 | 23,8 |
| Tremor and stiffness | 15 | 17,9 |
| Tremor, bradykinesia, and facial expressiveness | 12 | 14,3 |
| Tremor, bradykinesia and postural instability | 8 | 9,5 |
| Tremor at rest and movement | 7 | 8,3 |
| Tremor of rest | 5 | 6,0 |
| Bradykinesia | 5 | 6,0 |
| Others | 6 | 7,2 |
| Affected limbs (n=84) | (n) | (%) |
| All members | 28 | 33,3 |
| Right upper and lower limbs | 16 | 19,0 |
| Upper and lower left limbs | 15 | 17,9 |
| Both upper extremities | 9 | 10,7 |
| Left upper limb | 6 | 7,1 |
| Right upper limb | 4 | 4,8 |
| Upper right and lower left extremities | 3 | 3,6 |
| Others | 3 | 3,6 |
Tabla 3. Non-motor symptoms and comorbidities of patients with Parkinson's disease from the Ramiro Prialé Prialé Hospital of Huancayo.
| Non-motor symptoms (n=56) | (n) | (%) |
| Sleep disturbances | 32 | 38,1 |
| Thought disturbances | 9 | 10,7 |
| Thought and sleep disturbances | 8 | 9,5 |
| Language alterations | 3 | 3,6 |
| Thought alterations, sleep and language | 2 | 2,4 |
| Memory disorders | 2 | 2,4 |
| Autonomic symptoms (n=27) | ||
| Sialorrhea | 16 | 19,0 |
| Gastrointestinal disorders | 7 | 8,3 |
| Orthostatic hypotension | 4 | 4,8 |
| Urinary symptoms (n=58) | ||
| Urge to urinate | 32 | 38,1 |
| Nocturia | 21 | 25,0 |
| Increase in frequency | 5 | 6,0 |
| Sensory symptoms (n=84) | ||
| Pain | 61 | 72,6 |
| Ageusia | 9 | 10,7 |
| Pain and akatisia | 9 | 7,1 |
| Pain and paresthesia | 4 | 4,8 |
| Paresthesia | 4 | 4,8 |
| Treatment (n=80) | ||
| Levodopa - carbidopa | 43 | 51,2 |
| Levodopa | 37 | 44,0 |
| Additional treatments (n=81) | ||
| Anticholinergics | 51 | 60,7 |
| Anticholinergics and selegiline | 11 | 13,1 |
| Selegiline and/or other antidepressants | 8 | 9,5 |
| Anticholinergics and dopaminergic agonists | 7 | 8,3 |
| Dopaminergic agonists and selegiline | 4 | 4,8 |
| Family history of Parkinson's disease (n=84) | 18 | 21,4 |
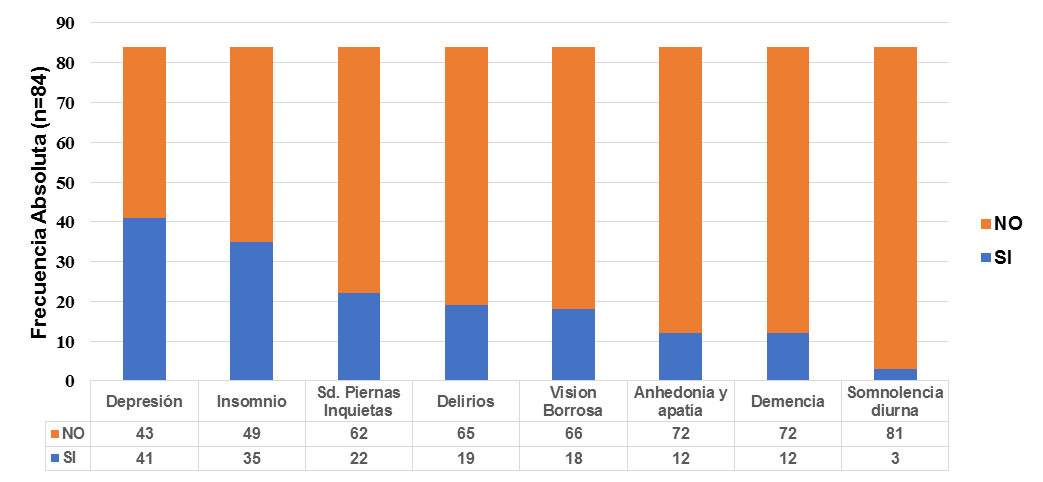
Figura 1. Comorbidities present in patients with Parkinson's disease at the Ramiro Prialé Prialé Hospital of Huancayo (Absolute frequencies)
DISCUSSION
In our study the average age was 72.93 years, the most frequent gender was male (58.3%) and the most prevalent levels were the degree of university education (50%) and secondary (27.4%). Similar results were found in Ecuador, the average age was 62.3 years and predominated in males (53.8%)11.In Chile, it also predominated in the male gender (58.73%) and the average age was 71.77 years, but we found a difference regarding the level of education, where patients without higher education represented 58.73%12. In another study carried out in Peru, there were important statistical differences in terms of the frequencies found with respect to the male gender (28.6%) and the average age (55.95 years)8.
In the clinical characteristics, we identified that regarding the duration of the disease, more than half had between 1 and 7 years.The most frequent motor symptoms were described as tremor at rest and bradykinesia. According to Martín13, he determined that the length of illness of patients with Parkinson's disease was 7.36 years. The National Institute of Neurologic Sciences (INCN) established that 42.86% had a time of illness between 5-9 years and that the most prevalent motor symptoms in order of highest to lowest frequency were: bradykinesia (87.3%), stiffness (84.16%), tremor (79.37%) and postural alteration (74.6%)14. In the same line Cuba J, et al., in the characterization of motor symptoms the condition in patients who were younger than 40 years had a unilateral alteration, being the condition of the upper limb (65.30%), and the lower limb (34.7%)8.
Núñez-Peralta15, reports that the most frequent motor symptoms are stiffness (69.4%), tremor (64.2%) and bradykinesia (42.5%) and non-motor symptoms sleep disorders (38.1%) and urge to urinate (38.1%). In addition, the use of anticholinergics predominates (60.7%); 21.4% reported having a family history of Parkinson's disease and the most frequent comorbidities were depression (48.8%) and insomnia (41.7%). Según Navarro16, in the pharmacological treatment of these patients, the combination of dopamine and other antiparkinkinin drugs was present in 52.5%. Regarding the history of Parkinson's disease, there were differences with the study conducted in Chile, where possibly being a specialized institution they determined that 100% of their patients had a family background12, , in our study only a fifth had a history (21.4%), it is important to study the "Mitochondrial Dynamics" in certain patients, Although it is generally known that in the vast majority of patients with Parkinson's disease there is a multifactorial component17,18.
Regarding the neuropsychiatric comorbidities associated with Parkinson's disease, Martin13 Martin13 identified in his study the presence of dementia (12%), sleep disorders (81.36%) and depression (37.1%). In our country it was identified that among the complications that these patients develop depression is very frequent (42.85%)8,19,20; Núñez-Peralta15determined, in the non-motor symptoms, that depression was present in 26.9% of the patients.
The limitation of our research work is that being an observational, retrospective and case series study, we only describe the characteristics of this group of patients with Parkinson's disease, which probably does not generate evidence that allows us to alter clinical practice, except its epidemiological surveillance and know the clinical picture, moreover be able to evaluate the best methodology for further research.
CONCLUSION
It was determined that Parkinson's disease is a pathology that mainly affects older males, the most characteristic motor symptom is tremor and bradykinesia and non-motor symptoms sleep disorders such as insomnia and depression.
Authorship contributions: the authors participated in the genesis of the idea, project design, data collection and interpretation, analysis of results and manuscript preparation of the present research work.
Financing: self-financed.
Conflict of interest: the authors declare no conflict of interest in the publication of this article.
Received: March 20, 2019
Approved: August 29, 2019
Correspondence: Joel Atencio
Address: Av. Manantial 4817, Sapallanga- Huancayo; código postal: 12000
Telephone: 927999363
Email: yoel_005@yahoo.com
REFERENCES
