REPORTE DE CASO
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2019 - Universidad Ricardo PalmaDOI 10.25176/RFMH.v19i4.2346
UNDIFFERENTIATED CARCINOMA WITH OSTEOCLAST-LIKE GIANT CELLS (UC-OGC) OF THE HEAD OF PANCREAS.
CARCINOMA INDIFERENCIADO CON CÉLULAS GIGANTES DE TIPO OSTEOCLASTOS EN LA CABEZA DE PÁNCREAS.
Eugenio Palomino1,a,
Jesús E. Talavera2,3,b
1 Edgardo Rebagliati Martins National Hospital. Lima, Peru
2 Research Institut in Biomedical Sciences, Ricardo Palma University. Lima, Peru.
3 Peruvian Institute of Celular Engineering and Tissue Manufacturing. Lima, Peru C. A. Lima, Peru.
a Pathologist
b Medicine student
ABSTRACT
Undifferentiated carcinoma with undifferentiated osteoclast-like cells (UC-OGC) in the head of the pancreas is extremely rare. The clinical-pathological, imaging and topographic appearance characteristics are not well classified. This case report describes a patient with UC-OGC of the Pancreas Head. Our patient, an adult over 75 years of age, had a considerable illness time, without relevant symptoms until the advanced stages of the tumor, debuting with shallow gastric discomfort, then weight loss. In the diagnostic tests they found the presence of a tumor that compromised the stomach, duodenum and pancreas. The definitive diagnosis was given by the pathological study. There are not enough clinical data available for a treatment that guarantees a higher survival rate in patients, however, pancreatoduodenectomy is currently the alternative that offers the best results, on the other hand, the prognosis after surgery and the recurrence rate still uncertain.
Keywords: Carcinoma, Giant Cell; undifferentiated carcinoma, pancreas, pancreas head (Source: MeSH)
RESUMEN
El carcinoma indiferenciado con células indiferenciadas tipo osteoclasto (UC-OGC) en cabeza de páncreas, es extremadamente raro. Las características clínico-patológicas, de imagen y la apariencia topográfica no están bien clasificadas. Este reporte de caso describe un paciente con UC-OGC de Cabeza de páncreas. Nuestro paciente un adulto mayor de 75 años de edad, presentaba un tiempo de enfermedad considerable, sin sintomatología relevante hasta las etapas avanzadas del tumor, debutando con molestias gástricas someras, luego pérdida de peso. En los exámenes diagnósticos hallaron la presencia de un tumor que comprometía el estómago, duodeno y páncreas. El diagnóstico definitivo lo dio el estudio anatomo-patológico. No se dispone de datos clínicos suficientes para un tratamiento que garantice una mayor tasa de supervivencia en los pacientes, sin embargo, la pancreatoduodenectomía es actualmente la alternativa que mejores resultados ofrece, por otra parte, el pronóstico después de la cirugía y la tasa de recurrencia sigue incierto.
Palabras Claves: Carcinoma de Células Gigantes, Carcinoma indiferenciado, páncreas, cabeza de páncreas (fuente: DeCS).
Undifferentiated carcinoma with giant cells of the osteoclast type (UC-OGC) located in the head of the pancreas is very unusual with few cases reported so far. It is one of the less common types of exocrine pancreatic tumors1,2. This pathology accounts for less than 1% of all pancreatic malignancies and was first described by Rosai 3 (6). It is characterized by the presence of two cell populations: undifferentiated polymorphic mononuclear epithelial cells and benign multinucleated giant cells.
The clinical-pathological and imaging characteristics and tomographic appearance are not well defined5. In addition, the pathogenesis and histogenesis of these tumors is highly discussed.
Here is a case that describes a patient with pancreatic head UC-OGC.
REPORT OF THE CASE
We describe the case of a 75-year-old male patient from Lima with no significant personal history. He has a time of illness of 2 and a half months, of insidious start and progressive course. He has abdominal pain in epigastric, oppressive, with progressive intensity that worsens with food intake. Days later, the condition is exacerbated by melena episodes and weight loss (approx. 8kg since the onset of his illness). For this reason, he goes to a nearby health center. He is evaluated and a pancreatic tumour is evidenced in Computerized axial tomography. The patient is referred to the Edgardo Rebagliati Martins National Hospital.
At the time of admission, the patient was awake, pale, and thin. The physical examination revealed only a hard abdominal mass, painful to palpation, with irregular epigastric edges of approximately 15x10 cm. The rest of the physical examination showed no further alterations. In the auxiliary exams: Hemoglobin 7.0 g/dl (VN: 13-16 g/dl), Abastonados 0%, Albumin 2.55 g/dL (VN: 3.5 -5 g/100mL), Creatinine 1.05 g/dL (VN: 0.5 [ 1.3 mg/dL), Urine coagulation, biochemistry within normal values. Inflammatory Markers: PCR 2.48 mg/dL, VSG 33 mm. Tumor markers: CA 19-9 in 14 U/mL, CEA 4.3 ng/mL, AFP 1.8 ng/mL. The high digestive endoscopy is described extrinsic compression in the minor curvature and anterior wall of the gastric body; the pylorus is permeable, through it is observed polypoid lesion that protrudes its light at the level of the duodenal bulb; in the duodenum was observed a wide polyploid lesion occupying bulb and first portion of it (approx 5cm), also the presence of an ulcerated lesion in proximal end of regular, friable and soft surface at the biopsy; base is not identified and the mucosa is erythematous. Based on the clinical history and the examinations carried out, it is concluded that the patient has a subepithelial lesion in the duodenum, to rule out a pancreatic tumour.
In the imaging studies carried out from the 3rd day of admission to the internal medicine service were: The first Computerized axial tomography test carried out concluded that the tomographic findings show suggestive lesion of Malignant Neoplasia of the head of the pancreas, which impacts and displaces the gastric antrum, first and second portion of the duodenum and probably infiltrates them, conditioning dilation of the Wirsung conduit, in addition to free right subphrenic fluid in small quantity (Fig. 1). The third Computerized axial tomography scan performed 20 days later shows: Pancreas with solid heterogeneous cystic lesion, 9x5.3 cm, located in the neck and body of the gland that compresses the gastric body, expands the duodenal frame that has neoformative appearance. No free fluid in the abdominal cavity. Prostate prominence (Fig. 2).
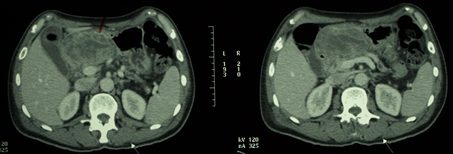
Figure 1: Pancreas with extensive solid neoformative lesion dependent on the head, measures 4.8x7.7cm, anteroposterior and transverse, has partially defined edges, contact with the gastric antrum as well as with the first and second portion of the duodenum, not existing an adequate differentiation with these structures probably infiltrates them, the pancreatic body and tail are atrophic with Wirsung dilation..
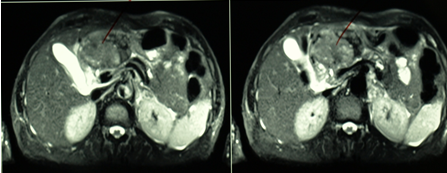
Figure 2. El páncreas muestra una extensa lesión solida quística heterogénea de 9x5.3cm The pancreas shows an extensive solid heterogeneous cystic lesion of 9x5.3cm located in the neck and body of the gland, conditions dilation and distal atrophy, compresses the gastric body, enlarges the duodenal frame, has a neoformative aspect.

Figure 3: Macrophotograph of the specimen, observing distal stomach, first its second duodenal portion and gallbladder with extrahepatic bile duct. Highlights an exophytic neoplasia, deforming the duodenum and distal stomach, irregularly oval, of 7.5cm of greater diameter, with areas of brown, black and greyish color.
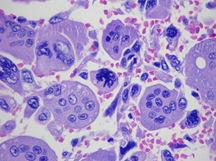
Figure 4A: Two distinct cell populations are observed: the cells of undifferentiated carcinoma, with marked anaplasia and atypical mitosis. The other population corresponds to the giant multinucleated osteoclast cells, of benign, reactive nature. (Coloration H-E, 400 X).
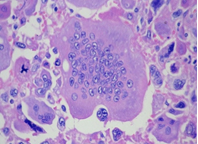
Figure 4B: A giant multinucleated osteoclast phagocyte cell with an undifferentiated neoplastic cell of carcinoma, with 3 pleomorphic nuclei and loss of the nucleus-cytoplasm relationship. (Colour H-E, 400 X).
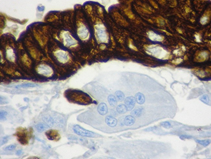
Figure 4C: Immunohistochemistry test for Cytkeratin, demonstrating the epithelial nature of the malignant cell population. The giant multinucleated cell is negative. (Coloration H-E, 400 X).
Our patient, an adult over 75 years of age, presented a considerable time of illness without presence of relevant symptoms until the tumor was in advanced stages, debuting with shallow gastric discomfort, moving on to weight loss. Diagnostic tests suggested the presence of a tumor involving the stomach, duodenum, and pancreas. And the subsequent anatomical-pathological study gave the definitive diagnosis of this pathology. Undifferentiated carcinoma with giant cells type osteoclast of pancreas, is a very rare neoplasia. It is listed in the Classification of Pancreatic Tumors by the World Health Organization in its 2010 edition6.
This pathology is characterized by the presence of two cell populations: undifferentiated polymorphic mononuclear epithelial cells and benign multinucleated giant cells. Nodal involvement and metastases are unusual, however, neoplasia often invades adjacent structures. It has been reported that the average survival in these cases is 11 months7.
There are few cases in the literature and no cases have been reported in Latin America. The male-female prevalence is 2:3 and the average age is 67 years with a range of 33 to 88 years (8). This type of tumor can be located in different organs, in the digestive system its most frequent location is the gallbladder and pancreas8. In our patient imaging studies suggested the presence of tumor located in the head of the pancreas with extension to the muscularis mucosae of the adjacent duodenum, whose initial diagnosis was delayed due to the atypical presentation of the clinical picture and the scarcity of similar cases.
The clinical presentation of this pathology is usually associated with abdominal pain, palpable mass, weight loss, fatigue, anorexia and jaundice9. Commonly located in the body and tail of the pancreas4, in our case the tumor was located in the head of the pancreas. The differential diagnosis of this pathology includes cystic lesions, such as ductal pancreatic carcinomas or neuroendocrine tumors10. In our patient the most important clinical findings were abdominal pain and weight loss. There is currently no specific information on the clinical course or guidelines for the management of this pathology. Even adjuvant treatment with chemotherapy is not fully established4, however radiation therapy has been applied as a basis for the radio sensitivity of giant cell tumors of the bones to this.
The histological origin of UC-OGC is currently a subject of controversy since some postulates, using electron microscopy techniques, indicate that it originates from mesenchymal tissues11. Other authors suggest that the tumor originates from a precursor of pluripotential cells which have the ability to differentiate into specific phenotypes.4. In our patient the pathological anoatom report confirmed in fact the presence of component of osteoclast-type giant cells and fusocellular sarcomatoid component.
In the present case the patient already had risk factors mentioned above, however, the initial symptomatology is very unspecific, making the only current means for diagnosis the pathological anoatom study. Currently the guidelines on management and prognosis are not clear, however a poor prognosis is recognized with the death of the patient within a few months of diagnosis12. Added to this, some poor prognostic factors are identified as advanced age, male sex, small tumors, positive metastases and a concomitant component of ductal adenocarcinoma13.Our patient had some of the previously mentioned factors of poor prognosis, after the surgical resection of the tumor the follow-up of the patient was lost; however literature describes that this type of tumor has a considerable rate of recurrences14.Subsequently the patient is alive, and at the moment show no signs of tumor recurrence after surgery. This suggests that pancreatoduodenectomy offers the best results for the treatment of this type of tumor. There is no standard chemotherapy, however, most case reports used gemcitabine as maintenance therapy. Therefore it is necessary to study more similar cases, compare them, continue with long-term follow-up and evaluate the effectiveness of pancreatoduodenectomy in this type of patients in order to obtain more data on the clinical course of the disease, guidelines on their handling and more precise data on their treatment and prognosis in these patients.
CONCLUSION
Undifferentiated carcinoma with giant cells of the osteoclast type is a rare type of tumor and because of this, there are not enough clinical data available for a treatment that guarantees a higher survival rate in patients. However, pancreatoduodenectomy is currently the alternative that offers the best results, on the other hand, the prognosis after surgery and the rate of recurrence remains unclear.
Authorship contributions: The authors participated in the generation, information gathering, writing and final version of the original article.
Funding: Self-funded.
Conflict of interest: The authors declare no
conflicts of interest in the publication of this article.
Received: July 20, 2019
Approved: September 7, 2019
Correspondence: Jesús E. Talavera
Address: Jr. Monte Cedro 413, Santiago de surco. Lima, Perú.
Phone number: (511) 959 706 046
E-mail: enrique7.talav@gmail.com
