ORIGINAL ARTICLE
JOURNAL OH THE FACULTY OF HUMAN MEDICINE 2020 - Universidad Ricardo PalmaDOI 10.25176/RFMH.v20i2.2916
PATIENT COMPLAINTS IN THE ADULT EMERGENCY DEPARTMENT OF A TERTIARY REFERRAL HOSPITAL
RECLAMACIONES DE PACIENTES EN EL SERVICIO DE EMERGENCIA ADULTOS DE UN HOSPITAL DE TERCER NIVEL DE ATENCIÓN
Isabel J. Alamo-Palomino1, Juan P. Matzumura-Kasano2,3
, Hugo F. Gutiérrez-Crespo2
1Oficina de Calidad, Red Prestacional Rebagliati – ESSALUD, Lima-Perú.
2Facultad de Medicina de la Universidad Nacional Mayor de San Marcos, Lima-Perú.
3Posgrado e investigación de la Universidad Nacional Mayor de San Marcos, Lima-Perú.
ABSTRACT
Introduction: The critical condition of the patient who presents to an emergency department creates a need to provide timely, safe and warm care. Failing to meet these expectations causes patient dissatisfaction, reflected by complaints, which are mostly justified and lead to opportunities for improvement and corrective measures.
Objective: To analyze complaints presented by patients and their relatives at the Adult Emergency Department of the Edgardo Rebagliati Martins National Hospital.
Methods: Nonexperimental, descriptive, cross-sectional study. Our sample was comprised of 109 complaints between May and November 2019. We used a data collection sheet based on the information in the complaints book for health care services.
Results: We identified 187 reasons for complaints. Our results show that direct relatives filed 47.7%; 43% involved Internal Medicine consultations. In the dimension “inadequate treatment by healthcare workers,” 13.9% of patients complained about impolite and rude treatment. In the dimension “delay in care”, 12.8% were discontent due to the lack of timely care. In the dimension “user disagreement with care or treatment received,” 10.2% were dissatisfied with the care they were provided. 60.6% of complaints were satisfactorily resolved within the period specified by current regulations.
Conclusion: Most complaints were related to the direct care of the patient.
Keywords: Patient; Emergencies; Attention Delivery of Health (source: MeSH NLM).
RESUMEN
Introducción: La condición crítica del paciente que acude a emergencia genera la necesidad de otorgar una atención oportuna, segura y cálida. No cubrir estas expectativas desencadena en la insatisfacción del paciente, reflejada mediante reclamaciones, las cuales en su mayoría resultan justificadas, generando oportunidades de mejora y medidas correctivas.
Objetivo: Analizar las reclamaciones presentadas por el paciente y sus familiares en el servicio de emergencia adultos del Hospital Nacional Edgardo Rebagliati Martins.
Métodos: Diseño no experimental, descriptivo, de corte transversal. La muestra estuvo conformada por 109 reclamaciones durante el periodo comprendido de mayo a noviembre 2019. Se utilizó una ficha de recolección de datos con la información del Libro de Reclamaciones en Salud.
Resultados: Se identificaron 187 motivos de reclamaciones. Los resultados mostraron que 47,7% fueron presentadas por familiares directos y que 43% correspondieron al área de medicina interna. En la dimensión inadecuado trato por parte del personal asistencial, 13,9% de pacientes mostraron disconformidad frente al trato descortés y grosero; en la dimensión demora en la atención, 12,8% manifestaron encontrarse descontentos por la falta de atención oportuna y, en la dimensión desacuerdo del usuario con la atención o tratamiento recibido, 10,2% quedaron insatisfechos con la atención recibida. 60,6% de reclamaciones se resolvieron satisfactoriamente dentro del plazo exigido en la norma.
Conclusión: La mayor cantidad de reclamaciones correspondieron al tipo prestacional, asociadas a la atención directa del paciente.
Palabras Clave: Paciente; Emergencia; Atención (fuente: DeCS BIREME).
The emergency service is the area in charge of providing timely and safe care to patients who seek emergency medical attention due to the critical health problem they present. In this area work different types of professionals and go a large number of patients. In recent years, the increase in demand and the deficient growth of supply cause patients to go through long waiting times to receive the care requested in these services, generating situations of stress, work overload in health professionals, delay in care, possible poor results in the care process and patient dissatisfaction(1). Going to emergency services is also stressful for the patient and their families, triggering an imbalance in the family nucleus, affecting them emotionally, which can alter their behavior and perception when facing an emergency situation(2).
It is important to emphasize that emergency services guarantee one of the fundamental rights of the population; On the other hand, trying to achieve universal health insurance has generated greater interest in improving the quality of care(3). . Knowing the expectations of the patient who comes to receive the health care, allows the facility to understand the needs and provide quality care, taking into account that a poor quality of care is associated with dissatisfaction, which produces a break in the doctor-patient relationship, generates a negative experience in the patient that can be transmitted to family members, damaging the image of the facility or expressed through complaints(4,5,6). In this sense, the patient's perspective is important, due to their sensitivity and ability to recognize a wide range of health care problems received, due to the different view they have of the problems compared to those reported by health personnel. Therefore, complaints provide important additional information to the health organization on how to improve care processes(7,8).
Patients who go to emergency services need to receive clear, consistent and complete information related to the health problem that motivated them to come, to resolve their doubts or concerns regarding the treatment, diagnostic or therapeutic procedure to which they are or will be subjected, to receive prompt, timely, safe and quality care, to receive at all times a warm and humane treatment, To be found in optimal environments that have the necessary infrastructure, equipment, materials and medicines to ensure care(9). When these conditions do not exist, complaints arise, which are key indicators of problems in the health system; For these reasons, they are now recognized as a valuable source of information on the care process and can be used positively to reflect on the practice and services provided, allowing opportunities for improvement to be established(10,11).
The analysis of complaints allows reflection and recognition of problems in patient safety, can be used effectively to identify adverse events through which the services involved develop and implement improvement plans to optimize the quality of care(12). However, it is important to emphasize that complaints do not have a standard classification, on the contrary, they are classified differently, in different health systems and in different countries, which creates problems when making comparisons and drawing conclusions, hindering the development of an approach as national policy(13). Therefore, research has been initiated to systematically examine the complaints of patients and their families, to understand and improve the communication skills of health personnel involved in the care process, to improve the safety and quality of clinical care, as well as the management of the health organization and to help repair problems in the doctor-patient relationship, helping to ensure patient satisfaction(14). Therefore, the objective of this study is to analyze the complaints of patients and their families in the adult emergency service of the National Hospital Edgardo Rebagliati Martins during 2019.
METHODS
This study was conducted using a non-experimental, descriptive, prospective cross-sectional design. The study population consisted of complaints registered in the health complaints book of the adult emergency service of the National Hospital Edgardo Rebagliati Martins. A non-probabilistic convenience sample was obtained, consisting of 109 claims during the period from May to November 2019; Complaints registered before and after the study period, those written in a confused or illegible manner and those from bodies other than the adult emergency service are excluded from the sample.
In order to collect the information, a data collection form was developed based on information from the Health Complaints Book approved by Supreme Decree N.º 002-2019-SA Regulations for the Management of Claims and Complaints of Users of the Administrative Institutions of Health Insurance Funds - IAFAS, Institutions Providing Health Services - IPRESS and Management Units of Institutions Providing Health Services - UGIPRESS, public, private or mixed15. The data included in the form were: date of complaint, name, gender, type of user, reason for complaint, area where the complaint occurred, personnel alluded to and date of response of the area responsible for the complaint.
Currently, there is no standard coding or taxonomy for claims, so we used the Kawakita Jiro method or affinity diagram to stratify the grounds for claims, through this method each claim was reviewed and assigned to one, two or more dimensions, according to the content, obtaining nine dimensions: Patient's disagreement with the care or treatment received, delay in care, inadequate treatment by the assistance staff, inadequate treatment by the administrative staff, delay in administrative processes, inadequate environment, shortage of resources, poor communication, and others.
The content validity of the data collection form was carried out through a judgment of experts, calling six experts, obtaining a Kappa coefficient with a result of 0.78. The reliability was evaluated by the test retest method which involved the application of the same card twice to the same person, leaving a time interval between the test and the retest, obtaining the result of 0.73. For data processing, the SPSS version 25 in Spanish was used to calculate absolute and relative frequencies of the variables of the study object and a descriptive analysis of the sociodemographic data was performed. The data were not used for their own benefit, it complied with the basic principles of ethics. The study was approved by the Research and Teaching Office, as well as by the Ethics Committee of the National Hospital Edgardo Rebagliati Martins, ensuring the confidentiality of the information recorded.
RESULTS
During the study period, 109 complaints registered in the Health Complaints Book of the adult emergency service of the National Hospital Edgardo Rebagliati Martins were analyzed. The results show that 54.1% were women and 45.9% men. It was observed that 47.7% were presented by the patient's immediate family. Also, the analysis of complaints by dimensions showed that 23.5% correspond to inadequate treatment by the assistance staff followed by 23% for delay in care and 13.9% related to patient disagreement with the care or treatment received (Figure 1).
The results show that in each of the complaints there is more than one reason that generates the dissatisfaction of the patient or family, evidencing a total of 187 reasons were identified among the 109 complaints analyzed; Depending on its nature each motif was assigned to different dimensions. The results corresponding to the dimension patient disagreement with the care or treatment received, identified that 10.2% of patients disagree with the care received; Regarding the dimension delay in care, 12.8% complained about the lack of timely care; In the dimensions inadequate treatment by healthcare and administrative staff, it was found that 22% of complaints were due to inadequate treatment (discourteous and rude) by service staff. Regarding the dimension poor communication, 7.5% of patients reported that the reason for dissatisfaction was due to the poor quality of the information received; As regards the dimension delay in administrative procedures, 8.5% said that the reason for complaint was due to slow administrative procedures and the slow procedure in the area of admission, the latter being the most frequently described in complaints. The results obtained in the dimension inadequate environment, showed that 2.1% of patients are dissatisfied with the lack of comfortable environments; While in the dimension lack of supply of resources, 1.6% due to the lack of medicines in the pharmacy and in the last dimension others, 0.5% attributed the complaint to the lack of specialists in the emergency service (Table 1).
The analysis of the 187 reasons for complaints showed that 133 corresponded to problems of benefit type, associated with direct patient care and 54 administrative type. The months in which the highest number of claims were submitted were May and August, the same months in which administrative claims were presented in greater numbers (Figure 2).
In relation to the analysis of the frequency of complaints by areas of the adult emergency service of the National Hospital Edgardo Rebagliati Martins, it was observed that 43% occurred in the area of internal medicine, followed by 16.1% in the triage area and 9.7% in nursing (Figure 3).
In the review of the cases, 32.1% of complaints correspond to the dimensions of inadequate treatment by healthcare and administrative personnel, of which 66.7% refer to professional health personnel: doctors 40% and nurses 20% and 33.3% reported that the staff offering the first contact with the institution were security guards (15.6%), admissions officers (6.7%) and care personnel (4.4%).
With regard to the analysis of complaint resolution measured in days, it should be noted that the rule states that the maximum time for dealing with complaints should not exceed 30 working days. This study showed that 60.6% of complaints were satisfactorily resolved with an explanation or an apology; 69.1% within the first 10 days; 19.1% between 11-20 days and 11.8% between 21-30 days. While 39.4% of complaints were resolved after 30 days, exceeding the response period required by the current rule (Figure 4).
Table 1. Frequency of reasons for complaints recorded in the adult emergency health complaint book.
| Grounds for complaints | N | % | ||
| Direct Reasons | Dimension |
Patient’s disagreement with the care or treatment received Disagreement with the care received Disagreement with the treatment received Negligence or malpractices |
26 19 6 1 |
13,9 10,2 3,2 0,5 |
| Dimension |
Delay in care Prolonged waiting time in triage Lack of timely care Delay in carrying out procedures |
43 17 24 2 |
23 9,1 12,8 1,1 |
|
| Dimension |
Inappropriate treatment by healthcare personnel Inappropriate treatment by healthcare personnel Inappropriate treatment by healthcare personnel Lack of consideration by staff/dehumanization |
44 26 1 17 |
23,5 13,9 0,5 9,1 |
|
| Dimension |
Poor communication Poor communication about health status Insufficient information to family members Poor quality of information |
22 4 4 14 |
11,8 2,1 2,1 7,5 |
|
| Administrative reasons | Dimension |
Inappropriate treatment by administrative staff Inappropriate treatment (discourteous, rude) Inappropriate treatment (discourteous, rude) |
16 15 1 |
8,6 8,1 0,5 |
| Dimension |
Delay in administrative procedures Slow procedures on admission Delay in delivery of medicines Slow administrative processes Undefined administrative processes Delay in transfer to hospitalization Delivery of dinner is too late Failure to comply with opening hours in inadequate pharmacy |
24 6 1 10 3 2 1 1 |
12,8 3,2 0,5 5,3 1,6 1,1 0,5 0,5 |
|
| Dimension |
Inappropriate environment Uncomfortable environments Lack of privacy in environments Inadequate signage |
7 4 2 1 |
3,7 2,1 1,1 0,5 |
|
| Dimension |
Shortage of resources Lack of medicines in pharmacy Lack of wheelchair |
4 3 1 |
2,1 1,6 0,5 |
|
| Dimension |
Others Lack of specialist |
1 1 |
0,5 0,5 |
|
| Total | 187 | 100 | ||
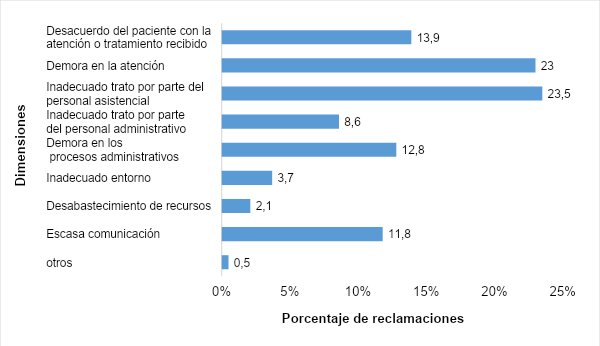
Figure 1. Analysis of claims for dimensions in the adult emergency service.

Figure 2. Distribution of claims of a direct and administrative type by months in the adult emergency service.

Figure 3. Analysis of frequency of complaints by adult emergency service areas

Figure 4. Analysis of frequency of complaints by adult emergency service areas.
The growing demand for health services is one of the elements that has favored the saturation in emergency services, this associated with the delay in care or the performance of diagnostic tests, procedures and therapy, generate a decrease in quality indicators such as unattended patients, long waiting times, prolonged stays, increased occurrence of adverse events, patient-family dissatisfaction and complaints. In addition, the saturation of emergency services has an impact on health personnel, manifested in work overload that leads to inadequate treatment, interpersonal conflicts and rupture in the doctor-patient relationship(16,17). Complaints are the result of unmet expectations of the patient or reflect poor quality of service. The analysis shows the existence of weak points that occur from the entry of the patient by triage until discharge from the service and, in turn, serves as a tool for improving perceived quality(18).
The results of the present study show that the inadequate treatment by the assistance personnel and the delay in the attention in the emergency service, continue to be the main reasons of dissatisfaction of the patient, reflected through complaints. These same motivations have been evidenced in another study carried out in a hospital in Australia, in which they point out the existence of three main reasons for complaints, such as inadequate treatment and diagnosis 16.9%, bad attitude or discourteous treatment 13% and delay in treatment due to long waiting times 11.9%, which ends up affecting patient and family satisfaction, communication and interpersonal relations(19,20).
The critical condition of the patient who goes to the emergency service should generate in the health professionals who intervene throughout the care process, the need to feel concern, empathy and respect for the patient(21). Although it is true, the above should be part of the idiosyncrasy of the health personnel, the analysis of complaints of the research study determined that, in many cases, there is more than one problem that motivates the dissatisfaction of the patient, the main one being the inappropriate, rude and discourteous treatment by the assistance personnel, especially associated with medical and nursing care. This is still a problem in state-run hospitals. Similarly, these findings have been evidenced in other studies, in which the perception of family members regarding the medical care received turns out to be unfavorable, reaffirming the need of the patient and his family to receive dignified treatment. Likewise, research conducted in Mexico through surveys showed that the care received by health personnel obtained worrying results, in which only a small group of patients surveyed said they were treated with dignity, while more than half reported that their rights as persons were never exercised(22,23).
Currently, health facilities work hard to disseminate the duties and health rights of patients, a fundamental condition for anyone to be able to enjoy timely care in cases of emergency; In an environment that has adequate infrastructure and essential minimum resources; Situation that has not been fulfilled in public hospitals in the health sector; Therefore, in this study, the lack of opportunity in care became the second problem evidenced by patients and their families, manifested through complaints. It is important to emphasize that this result not only corresponds to studies carried out in our country but has also been demonstrated in another research carried out in a hospital in Spain, in which the delay and the untimely care constituted the fourth cause of patient dissatisfaction due to two reasons, First because the patient's expectations were not met and second because the health problem for which they went to the emergency service was not solved immediately.(24).
According to Saizar(25), the increasing access to information drives the patient to remain informed about the process of his illness, diagnosis and therapy, on the other hand, the saturation of the emergency service has generated impersonalized attention, lacking information and communication, making the patient feel as if he were not heard and that health professionals do not understand the experience of pain from the perspective of the patient. The union of these two reasons generates in the patient questions about the process of care or therapy received, producing conflicts or complaints of disagreement with health professionals; Likewise, Mack et al.(26) report that, in health issues, patients and their families are prioritizing two issues that define adequate health care: the doctor-patient relationship and the communication and information provided by the doctor in relation to their health status. Under that same perspective, the results of the research study showed as a third reason for complaint, the patient's disagreement with the care or therapy received in the emergency that triggers a break in the doctor-patient relationship and in some cases can go as far as complaints of alleged medical negligence or malpractice.
Given the above, it is important to emphasize that the communication and medical information provided to patients and their families becomes a determining factor in the results of healthcare quality. Communication between the doctor, patient and family should be appropriate, timely and understandable, helping to provide clear information on the state of health, treatment, procedures, evolution and prognosis of the disease(27). In view of what has been described, the present study revealed another important reason for complaint, which is the poor communication about the patient's health status, as well as the insufficient information provided to family members and the poor quality of information, which, in many cases, ends up deteriorating the doctor-patient relationship. Therefore, it is important to note that a similar study conducted in critical areas revealed that a large number of patients rated as poor the explanation given by the doctor about the cause of the disease and similarly, rated as poor the explanation received about the recovery process from the disease and the information provided by the doctor regarding the urgency of receiving a medication or procedure with the patient's consent, This confirms that the difficulties that arise during the process of communication between the patient and health professionals continue to be a problem that affects several health facilities(28).
Regarding to the time taken to resolve complaints, it should be noted that public entities are obliged, according to the law, to respond to complaints within a maximum period not exceeding 30 working days, by means of physical or electronic means. The present study showed that a large number of complaints were satisfactorily resolved within the established period. In the same way, similar research shows that complaints filed by patients and their families are resolved within the period established by the current regulation, which allows health facilities to generate opportunities that contribute to improving the quality of care and in turn, prevent similar events from recurring, for which they must establish corrective measures(29,30).
During the research study there were some limitations such as a relatively small sample size. The vast majority of complaints are complex and in some cases may have been misclassified, leading to measurement bias. The grounds for complaints were classified on a case-by-case basis; However, in the absence of a standard taxonomy or classification, comparison with other national and international studies is difficult.
CONCLUSION
A large number of complaints were filed by the patient's immediate family members. Most of the complaints were of a direct type, associated with direct patient care, mainly due to problems with the treatment received by the medical and nursing staff and the delay in care. The area of internal medicine received the highest number of complaints. Most complaints were satisfactorily resolved by means of an apology or explanation, with a smaller proportion of complaints resolved outside the time limits established in the regulation.
Statement: I declare that the material contained in the manuscript has not been previously published or submitted to another biomedical journal.
Authorship contributions: The authors participated in the genesis of the idea, project design, data collection and interpretation, analysis of results and preparation of the manuscript of this research work.
Financing: Self-financed by the authors.
Conflict of interest: The authors declare that they have no conflict of interest in the publication of this article.
Received: October 22, 2019
Approved: March 17, 2020
Correspondence: Isabel J. Alamo Palomino.
Address: Av. San Felipe 1161. Dept. 401. Jesús María, Lima-Peru.
Telephone: (+51) 958 934 984
Email: Isabel.alamo7@gmail.com
BIBLIOGRAPHIC REFERENCES
