ARTICULO ORIGINAL
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2020 - Universidad Ricardo PalmaDOI 10.25176/RFMH.v20i3.3114
COMPARISON OF EARLY NON-PHARMACOLOGICAL INTERVENTIONS ON COVID-19 MORTALITY OF PERU AND THE UNITED STATES OF AMERICA
COMPARACIÓN DE LAS INTERVENCIONES NO FARMACOLÓGICAS TEMPRANAS EN LA MORTALIDAD POR COVID-19 DE PERÚ Y ESTADOS UNIDOS DE AMÉRICA
Pedro Fidel Grillo Rojas1,a, Roberto Romero Onofre1,a,b
, José Aldana Carrasco1,2,a,c
1 Universidad San Martín de Porres. Lima, Perú.
2 Universidad ESAN. Lima, Perú.
aSurgeon, Specialist in Health Administration.
bDoctor in Health Management.
cMaster in Health Services.
ABSTRACT
Introduction: The pandemic that has been developing globally has tested not only the different health systems of the world but also the economic models and governments in every country. Objective: To compare the non-pharmacological
interventions of early application in the displacement and the amplitude of the daily mortality curve per million; as well as calculating the cumulative mortality rates and the number of deaths avoided by CORONAVIRUS SARS-Cov2 between Peru
and the United States. Methods: The daily mortality rate per million from the first registration, the maximum peak and the amplitude of this rate, as well as the cumulative rate for both countries, was calculated and evaluated under
the difference-in-differences method, to estimate the death rate avoided per million. Results: Mortality per million in Peru was 0.061 and in the United States 0.069. The first peak day in Peru recorded mortality in order of 3,276 per
million inhabitants at 46 days, and in the USA it was 14.88 per million at 47 days. The difference in differences is equivalent to a rate of -164,193 deaths per million, in Peru with respect to the United States of America. Conclusion: The early implementation of non-pharmacological interventions, including quarantine, would be related to a lower daily mortality in Peru compared to the United States of America.
Keywords: Coronavirus Infections; Mortality; Social Isolation (source: MeSH NLM).
RESUMEN
Introducción: La pandemia que viene desarrollándose a nivel global, ha puesto a prueba no sólo a los distintos sistemas de salud del mundo, sino a los propios modelos económicos y gobiernos en cada uno de los países.
Objetivo: Comparar las intervenciones no farmacológicas de aplicación temprana en el desplazamiento y la amplitud de la curva de mortalidad diaria por millón; así como la tasa de muertes evitadas por COVID-19 entre Perú y Estados Unidos.
Metodología: Se evaluó la tasa de mortalidad diaria por millón desde el primer registro, el pico máximo y la amplitud de dicha tasa, así mismo se calculó la tasa acumulada para ambos países y se evaluó bajo el método de diferencia
en diferencias, para estimar la tasa de muertes evitadas por millón. Resultados: La mortalidad por millón en Perú fue de 0,061 y de Estados Unidos de 0,069. El primer dia pico en Perú registro mortalidad en orden de 3,276 por millón
de habitantes a los 46 días, y de EUA fue de 14,88 por millón a los 47 días. La diferencia en diferencias equivale a una tasa de -164.193 muertes por millón, en el Perú con respecto a los Estados Unidos de América. Conclusiones: La
implementación temprana de las intervenciones no farmacológicas, incluida la cuarentena, no se relaciona con una menor mortalidad ni desplazamiento del pico de mortalidad diaria por millón en Perú respecto a los Estados Unidos de América.
Palabras clave: Infecciones por coronavirus, Mortalidad, Aislamiento social (Fuente: DeCS BIREME)
On January 5, 2020, the World Health Organization (WHO) reported that as of January 3, 2020, 44 cases of pneumonia of unknown causes had been detected in China; Wuhan City, Hubei Province, of which 11 were severe and 33 were stable, also reported the closure of the Wuhan market for disinfection .(1)
In February 2020, the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19), made up of 25 specialists from China, Germany, Japan, South Korea, Nigeria, Russia, Singapore, United States of America (USA) and the WHO itself; submitted a report in which some recommendations were issued. These instructions enable the highest level of national protocols for response management using non-pharmacological public health measures like active research, immediate isolation, and case follow-up; population education; application of diagnostic tests and simulations with different scenarios of non-pharmacological interventions to prevent the chain of transmission. (2)
The pandemic that has been developing at a global level has tested not only the different health systems of the world but also the economic models and governments in each of the countries. In this context, we have seen with perplexity how countries with highly consolidated health systems and solid economic systems, such as some European countries and the USA, have been presenting figures of infection and very high mortality .(3)
On the other hand, mathematical models were developed, in order to be able to forecast the development of the pandemic in different countries and thus be able to measure the impact of the disease and the actions to be taken to reduce said impact. Thus, different strategies have been implemented in each country, among which are the intensive use of diagnostic tests to identify cases and initiate isolation or treatment actions and non-pharmacological actions such as social distancing, voluntary or compulsory confinement in homes; the suspension of classes in schools and universities, prohibition of meetings, the closing of borders, among others . (4)
The “Imperial College COVID-19 Response Team” published a report on March 29, 2020 (5), din which the response team presented a model of how mortality and demand for health services would behave, comparing the different interventions in isolation or their joint implementation for the United Kingdom and the USA, grouping these strategies into the following two main groups:
Suppression: The main objective is to reduce the basic reproduction ratio (R) to 1 or below 1.
Mitigation: Whose main objective is not to eliminate the transmission from person to person, but to reduce the impact on health using non-pharmacological interventions, drugs, and other health technologies, waiting for the development of herd immunity.
As of May 3, the existing information could give us a preliminary idea about the application of different strategies and make a comparison between them, using rates or ratios on the total population of the countries, which would give us a more adequate preliminary view of the results achieved by each country. For this reason, the objective of the present study was to compare the impact of non-pharmacological interventions of early application versus late application on the displacement and the amplitude of the daily mortality curve per million inhabitants; as well as the death rate avoided by COVID-19, in Peru and the USA.
METHODS
Design and setting
The ecological study, comparing national data on mortality at the time of implementation of non-pharmacological intervention measures with quarantine in Peru and the USA.
Population and sample
Population studies were carried out, using the population of Peru and the USA (6,7).
Variables and instruments
The independent variable is the timeliness of the implementation of quarantine non-pharmacological intervention measures in Peru and the USA; for this purpose, it was considered appropriate only if the interventions were given before the first recorded death.
The unobservable characteristics that differentiate each country remain unchanged during the period of time studied.
The dependent variable is the accumulated mortality per million people in each country. Four cut-off points were applied for each country:
1. First cut-off point: First mortality record (per million population).
2. Second cut-off point: Initiation of non-pharmacological quarantine interventions.
3. Third cut-off point: Peak of mortality during the evaluation period.
4. Fourth cut-off point: End of evaluation (May 3).
The time from the beginning to the day of the maximum mortality peak during the full period of the intervention was counted in days. To demonstrate the displacement of the peak of daily mortality, the time from the start of interventions to the peak of daily mortality for each country during the evaluation period was calculated.
Procedures
The data were extracted from the reports of the Centers for Disease Control and Prevention and General Directorate of Epidemiology of both countries (ECDC), from the following two sources (6,7):
GitHub - owid / covid-19-data: Data on COVID-19 (coronavirus) confirmed cases, deaths, and tests. Available at: https://github.com/owid/covid-19- data
Coronademic Pandemic (COVID-19) - Statistics and Research - Our World in Data.
The data was downloaded and harmonized in the MS Excel computer program, from which the corresponding graphs and statistical analyzes were performed.
Statistical analysis
Differences in time and the amplitude of the mortality curve per million were compared, the data observed at the peak of daily mortality per million in each country were subjected to an equation under the difference in difference methodology (2,7).
The comparison was developed under the following equation:
X = (Yt1-YT0) - (Yc1-YC0) = (Yt1- YC0) - (Yc1- YT0)
Where:
X = Impact in relation to the outcome of confirmed cases and reported deaths by coronavirus (COVID 19).
Yt1-YT0: Death rate per million at the end and at the beginning of the evaluation period in the country with the application of quarantine before the first report of death per million.
Yc1-YC0: Death rate per million at the end and at the beginning of the evaluation period in the country with the application of non-pharmacological interventions that include quarantine after the first report of deaths per million.
A sensitivity test was applied to the data from Peru, due to the probability of underreporting of deaths diagnosed by COVID-19, with an increase of 50%; 100% and 200% at the time of peak daily mortality per million for the comparison of peak amplitude.
Ethical aspects
Worked with population data, without directly affecting any subject in the present study.
RESULTS:
In the case of Peru, there is no data reported at the beginning of the quarantine, mortality data per million are reported as of the fourth day and stand at 0.061 per million inhabitants. The first recorded peak day was 46 days after the start of the quarantine in the order of 3,276 per million inhabitants. Starting on day 43 from the beginning of nonpharmacological interventions in Peru, there was a steady increase in mortality per million reaching 3,276 per million by day 46, followed by a decline in the rate by day 47 and 48.
On Day 1 since the beginning of non-pharmacological interventions, there is evidence of a report of 0.069 deaths per million in the United States. By day 47 since the first registration of deaths per million, an important increase in the mortality rate is observed, reaching 14.88 per million that day, and then decreasing significantly and maintaining a tendency to decrease towards the day 63 with a daily rate of 3,979 per million inhabitants.
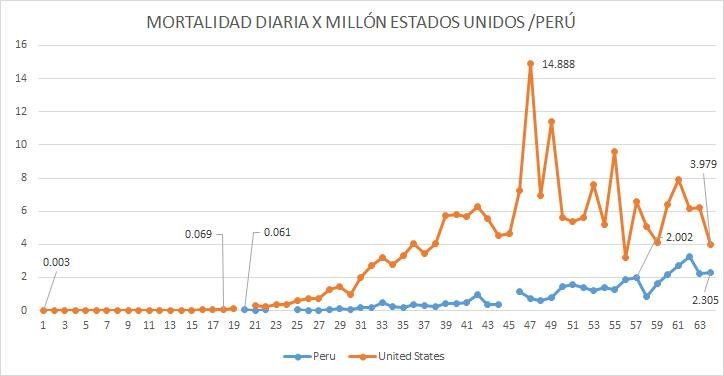
Fuente: ECDC, elaboración propia.
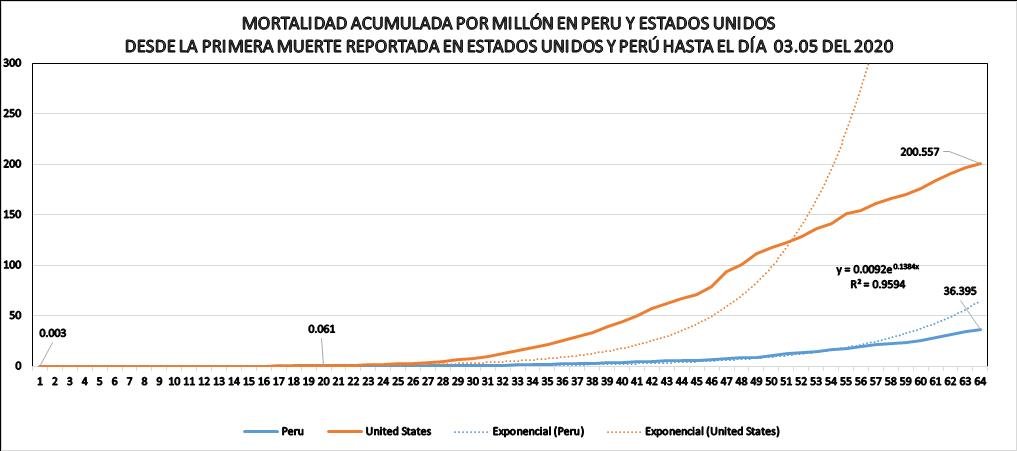
Fuente: ECDC Elaboración propia.
X= (36,95-0,061)-(200,557-0,03)= -164,193
Sensitivity analysis
In the assumption that in the United States there was no underreporting of mortality from COVID-19, various percentages of increase in cumulative mortality for Peru, evidence that even if there were an increase due to failures in the registration of 300%, there would be a rate of 98 deaths per million avoided in Peru compared to the United States of America.
Table 1. Sensitivity analysis of Peruvian data.
|
|
|
PERU |
U.S.A |
DD |
||
|
|
|
t1 |
t0 |
c1 |
c0 |
|
|
|
|
36,39 |
0,061 |
200,55 |
0,03 |
-164,19 |
|
PERCENTAGE INCREASE BY SUB-REGISTRY |
150% |
54,59 |
3,33 |
200,55 |
0,03 |
-149,26 |
|
200% |
72,79 |
4,44 |
200,55 |
0,03 |
-132,17 |
|
|
250% |
90,98 |
5,55 |
200,55 |
0,03 |
-115,08 |
|
|
300% |
109,18 |
6,66 |
200,55 |
0,03 |
-98,01 |
|
Countries correlated with the objective of non-pharmacological interventions of suppression, measuring the success or failure of these interventions by decreasing the reproduction ratio close to 1 or less than 1 during the course of the epidemic, however, the calculation of this ratio, in the specific conditions of Peru, with a changing number of tests carried out for the confirmation of the cases and unequal distribution of them at the regional level, which is why so far there is no official information on the ratio in quarantine conditions (8)
We believe that the use of mortality rates in the case of the current pandemic would easily express the positive or negative results of non-pharmacological interventions of suppression being directly related to the capacity of the system to absorb the demand, specifically in the emergency services, hospitalization, and intensive care units and measures directly the strain on these services in results of hospital discharges or deaths (6,7)
The application of non-pharmacological measures or interventions to control the transmission chain in the case of the current pandemic has been the subject of multiple interpretations and has been assumed differently by different countries in the world with mixed success. Italy, Spain, France, and the United States showed weak application, slow, and late interventions. These have generated a rapid increase in the curves of contagion and therefore of mortality, putting excessive pressure on the operational capacity of the health recovery services, mainly on hospitalization, and intensive care units causing high mortality and in the case of the United States very high (8)
In parallel, a collapse of the capacity of the morgues and funeral services including cremation services has been shown in these countries, which led in many cases to improvise morgues in container trucks, temporary cemeteries, and mass graves. The Elmhurst hospital was hit the hardest by the pandemic, which President Donald Trump cited on Sunday to explain his change of heart and the need for prolonged confinement. “I have seen things that I have never seen before, there are bodies in bags everywhere, in the corridors, they put them in refrigerated trucks because they cannot handle so many bodies. it's happening in Queens, in my community”, he said from the White House" (9-11)
The recommendations for the United States and Great Britain were specifically given on April 16, 2020. “The most effective combination conditioned on its duration is expected to be a combination of case isolation, home quarantine, and social distancing of those at greatest risk…in combination, this intervention strategy will reduce the maximum demand for critical care by two thirds and reduce the number of deaths by half. However, this optimal mitigation scenario would still result in an 8-fold spike in demand for critical care beds above the augmentation capacity available for both Britain and the United States” (12)
In the case of Peru we had access to an unpublished study developed by Jairo Pinedo et al., this work focused mainly on simulating different scenarios and how these scenarios influenced the ability of the system to absorb demand through intensive care units which concluded, “Mandatory social isolation (quarantine) until March 31 (scenario 6) or April 12 (scenario 7) followed by a combination of non-pharmacological interventions does not suppress or mitigate the epidemic and according to different scenarios could lead to the collapse of the health system with less or more delay. However, a strategy of compulsory intermittent social isolation separated by two months of non-pharmacological interventions would be successful by July of this year ” (13)
In this simulation scenario, 2 included a continuous quarantine "Perpetual Quarantine", which was rejected as an option because it was considered unfeasible. "Quarantine begins on March 15 and it is not suspended. The theoretical base Ro would be approximately 1, and there is a linear evolution of the disease. The health system does not collapse as the number of patients remains constant, ”but to date is the scenario that has actually been maintained, although the simulation results differ with what actually seems to have occurred in the country.
We have not been able to access any official projection that has served as a basis for the implementation of the suppression measures initiated in Peru on March 16, 2020.
Juan M. Cordovez et al. from the Universidad de Los Andes de Bogotá Colombia, developed a mathematical model for the city of Bogotá with the first conclusion that “The mitigation measures implemented allow to postpone the exponential growth of infections, but do not prevent the bed capacity in ICU. However, they are key to the preparation stage of the emergency and health systems ” (14)
The predictive models to which we have had access using different duration times of non-pharmacological interventions have agreed that these should be given in a combined manner that these measures are effective in reducing stress on health systems. There are divergences in relation to the amplitude of the peak of infections. However, the restrictions have no effect on the amplitude of the peak of infections observed over time. In the case without any restriction, the peak occurs until June 8, for each increase in the restriction of adult mobility in addition to the closure of schools and universities for 24 days between March 20 and April 13, it produces a postponement in the peak of up to 4 weeks in the case of restricting 100% of mobility ”(15-17)
In relation to the occupancy rate of the intensive care units “The closure of schools and universities combined with the restriction of adult mobility, slows down the infection rate. Increasing the duration of the restriction from 24 to 50 days has considerable effects on the rate. In the simulations, 100% of the people were restricted during the periods of time considered ” (18) , ),“ Although there are many uncertainties in the effectiveness of policies, this combined strategy is the most likely to ensure that requirements for beds in critical care remain within surge capacity” (11).
In accordance with what has been described by different authors regarding the stress on critical care, it is our opinion that it effectively eases the pressure on the beds in the intensive care units or critical units and it is essential to achieve better results in mortality from COVID -19.
The results of the present study would confirm the relationship foreseen in the hypotheses established in the three mathematical models. These were mentioned in the implementation of the combined measures of non-pharmacological interventions, including home quarantine, which would decrease the stress on critical care services and would be expressed in lower mortality during the period of implementation of these measures.
The novelty of this article shows that not only the application of non-pharmacological interventions is important, but the application before the first deaths happened.
Regarding the capacity of beds and health personnel, the situation in the United States is 2.9 per 1,000 inhabitants, while in Peru it is 1.6 per 1,000 inhabitants (5), This shows a better preparation of the United States against the development of the epidemic against Peru. However, the data would show that despite having better conditions, the results have not been favorable in the United States (18)
However; We are not certain in the case of Peru that this period has allowed us to increase the response capacity to face a possible wave after the quarantine was lifted.
In the United States of America, interventions that included social isolation either under compliance or on a voluntary basis (“shelter in place” or “stay at home”) were started gradually in different states. While the epidemic was in the process of spreading, there was a significant number of infected people and there were already counted deaths at the national level; as shown in the graph of mortality per million in the United States at the beginning of quarantines under any of the modalities, with San Francisco being the first city to implement it (19)
In most cases, both in Peru and in the United States, these interventions involved a different extent of restriction in the so-called non-essential activities, domiciliary social immobilization, transit restriction, closure of international or national borders in the case of Peru, isolation of cases and contacts, among other measures.
Peru began quarantining on March 16, 2020 (16,17), with no deaths reported, however, the weakness of this measure in our country is related to dissimilar compliance in different regions and even in different districts of the same city of Lima. The “Curfew” measure (20)had to be implemented at the national level as a measure of compulsory social immobilization due to the repeated non-compliance with quarantine by the population. It started at 8 in the evening and then from 6 in the afternoon on a national level and from 4 in the afternoon in some regions (21)
Both in the case of Peru and the United States, the performance achieved has not satisfied public opinion, politicians, and part of the health and scientific community.
Another weakness that we have identified in the process in Peru is related to Informal Labor, often dependent on daily earnings. The low level of balkanization of vulnerable populations was causing an agglomeration of people at the national level during the delivery of aid bonds issued by the government and the economic precariousness of migrant families, especially in Metropolitan Lima.
The so-called de-escalation process (removal of quarantines) in many countries has already started and in Peru, the removal is expected in May (15).
Within the limitations of the study, it is found that because population data was used, it is not possible to establish a direct correlation between non-pharmacological measures and mortality, but rather an inference that could indicate a relationship between these variables.
CONCLUSION
It is concluded that at the time of the end of the study it was not possible to establish a relationship between the early implementation of non-pharmacological interventions including quarantine or any of its variants. It would be related to a statistically relevant shift in the daily mortality peak per million in Peru compared to the United States of America during the evaluation period.
On the other hand, the early implementation of non-pharmacological interventions, including quarantine, would be associated with a lower mortality per million inhabitants in Peru compared to the United States. Peru had a rate of 164 deaths prevented per million inhabitants during the study period in relation to the United States of America. Once the quarantine is over, it is necessary to continue maintaining the other non-pharmacological interventions in a combined manner and to monitor confirmed cases, hospital admissions, and mortality, in order to develop focused or general interventions aimed at interrupting the transmission chain, until more evidence regarding drug treatments and vaccine are discover.
Authorship contributions: The authors participated in the genesis of the idea, project design, data collection and interpretation, analysis of results, and preparation of the manuscript of the present research work.
Financing: Self-financed..
Conflict of interest: The authors declare that they have no conflict of interest.
Received: May 18, 2020
Approved: June 19, de 2020
Correspondence: Roberto Romero Onofre.
Address: Instituto de Investigación en Ciencias Biomédicas, Facultad
de Medicina Humana, Universidad Ricardo Palma, Lima-Perú.
phone number: +511 980 222 114
e-mail: carlosromeroonofre@hotmail.com
REFERENCIAS BIBLIOGRÁFICAS
