REPORTE DE CASO
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2021 - Universidad Ricardo Palma10.25176/RFMH.v21i4.4041
ATRIAL FIBRILLATION THAT REQUIRED CARDIOVERSION IN THE POST ANESTHETIC RECOVERY UNIT IN AMBULATORY SURGERY. A CASE REPORT
FIBRILACIÓN AURICULAR QUE REQUIRIÓ CARDIOVERSIÓN EN LA UNIDAD DE RECUPERACIÓN POST ANESTÉSICA EN CIRUGÍA AMBULATORIA. UN REPORTE DE CASO.
Céspedes Morón Miryam1,a,b, Ruiz Roque Rosina1,2,b, Chipa Ccasani Fredy1,3,c
1 Clínica Internacional, San Borja, Lima - Perú.
2 Instituto Nacional Cardiovascular “Carlos Alberto Peschiera Carrillo” INCOR.
3 Hospital Nacional Guillermo Almenara Irigoyen
a Magister in Health Services, Magister in Medicine,
b Anesthesiology and Cardiovascular Intensive Therapy,
c Cardiologist Electrophysiologist
ABSTRACT
In recent years, the profile of patients who can undergo ambulatory surgery procedures in independent ambulatory surgical centers has changed. It is very important to consider the availability, skills and experience of the care staff, as well as the integral study of the patient, the resolution capacity of these centers and evaluations with quality care indicators to obtain optimal results. The present case was of a 34-year-old male, first presentation of rapid and symptomatic atrial fibrillation documented in the immediate postoperative period. Patient care, diagnostic strategy and treatment were described, since the patient required electrical cardioversion.
Keywords: atrial fibrillation, electrical cardioversion, otorhinolaryngology surgery, outpatient surgery (Source: MeSH NLM).
RESUMEN
Durante los últimos años, ha cambiado el perfil de los pacientes que pueden someterse a procedimientos de cirugía ambulatoria, en centros quirúrgicos ambulatorios independientes. Es muy importante considerar la disponibilidad, competencias, flujos de atención del personal asistencial, asimismo el estudio integral del paciente, la capacidad resolutiva de dichos centros y las evaluaciones con los indicadores de calidad de atención, para obtener así resultados óptimos. El presente caso fue de un paciente de sexo masculino, de 34 años de edad quien presentó por primera vez fibrilación auricular rápida y sintomática, documentada en el postoperatorio inmediato. Se describe la atención, la estrategia diagnóstica y el tratamiento, ya que requirió cardioversión eléctrica.
Palabras Clave: fibrilación auricular, cardioversión eléctrica, cirugía otorrinolaringología, cirugía ambulatoria (Fuente: DeCS BIREME).
INTRODUCTION
Outpatient surgery is a modern, comfortable, safe, innovative and economical procedure that allows the patient to quickly and effectively resolve a surgical inconvenience and return home the same day of surgery. 70-80% (1) of medium and low complexity surgical procedures can be solved in ambulatory surgery centers, (1) thus avoiding nosocomial exposure, achieving resource optimization (cost reduction by up to 40%), reducing bed occupancy. However, patients who undergo surgery with greater comorbidities are more frequent. Unexpected adverse events may occur in young patients, such as this clinical case where the patient developed atrial fibrillation, half an hour after his stay in the post-anesthetic recovery unit. This case occurred in Clínica Internacional in Lima-Peru.
Clinical case
34-year-old male, mixed race, from the city of Lima, with fibromyalgia history, allergic
rhinitis, undergoing rhinoplasty at 17 years of age, with a diagnosis of secondary septal deviation,
left valve collapse and hypertrophy of inferior turbinates, which was scheduled for otorhinolaryngology
surgery: ablusive septoplasty, plus bilateral turbinectomy with valvuloplasty. The patient received
total intravenous general anesthesia (propofol and remifentanil), TIVA-TCI (total intravenous
anesthesia-target control, infusion - goal-controlled anesthesia).
Clinical picture: Patient who in the Post-anesthetic Recovery Unit presented anxiety, referred
dyspnea, tachycardic palpitations.
Malampatti I airway exam, good oral opening and cervical mobility, thyromental distance, grade I
and Class I bite test.
Physical Exam: Pale skin and mucous membranes, devices and systems within normal limits.
Laboratory exams:
Hb15mmHg, Htco 45, leukocytes 4870, platelets 248,000, Group A +, TC 7, 'TS 2,' Glucose 93mmHg,
Urea 29, Cr 0.9, Serological negative.
ASA II, Surgical Risk I, elective surgery.
During the intraoperative period, it is monitored with a 5-lead ECG (electrocardiogram),
non-invasive blood pressure, oxygen saturation, capnography and monitoring of anesthetic depth, with the
index qCon values 40-60 and the nocioceptive stimulus with the qNox values 40-60.
A surgical checklist is performed, pre-oxygenation is carried out, objective-guided total
intravenous anesthesia was used, anesthetic induction was with Remifentanil 4ug./ml, propofol 2.5
ug./ml., With the mathematical models: MINTO for remifentanil and Marsh for Propofol, neuromuscular
relaxation was with Rocuronium 0.6 mg./Kg., in the maintenance of anesthesia Propofol and remifentanil
were used, according to site-effect objectives, cerebral anesthetic depth monitoring and non-invasive
hemodynamic monitoring. Controlled mechanical ventilation parameters were carried out according to
institutional protocols. The surgeon infiltrated lidocaine / adrenaline in the surgical area, showing no
arrhythmias. During the surgery he was hemodynamically stable, he did not register cardiac arrhythmias,
the surgical time was 2 hours 10 minutes.
As final analgesics he received Paracetamol 1gr. and tramadol hydrochloride 1-2mg / Kg. The
surgical anesthetic act proceeds without complications, the patient is extubated and for reversal of
neuromuscular relaxation, sugammadex 2mg / Kg is placed. The patient is taken to the Post-anesthetic
Recovery Unit awake, calm, with stable vital functions, painless and collaborative.
In the immediate postoperative period, approximately half an hour after his stay in recovery,
the patient suddenly becomes anxious, referring to dyspnea, tachycardial palpitations, without
hemodynamic decompensation. The cardiac monitor showed supraventricular tachycardia, an irregular pulse
of 143-160 bpm. A 12-lead electrocardiogram was performed and a cardiological evaluation was requested.
Transthoracic echocardiography showed normal structures, preserved left ventricular function, and no
intracavitary thrombi.
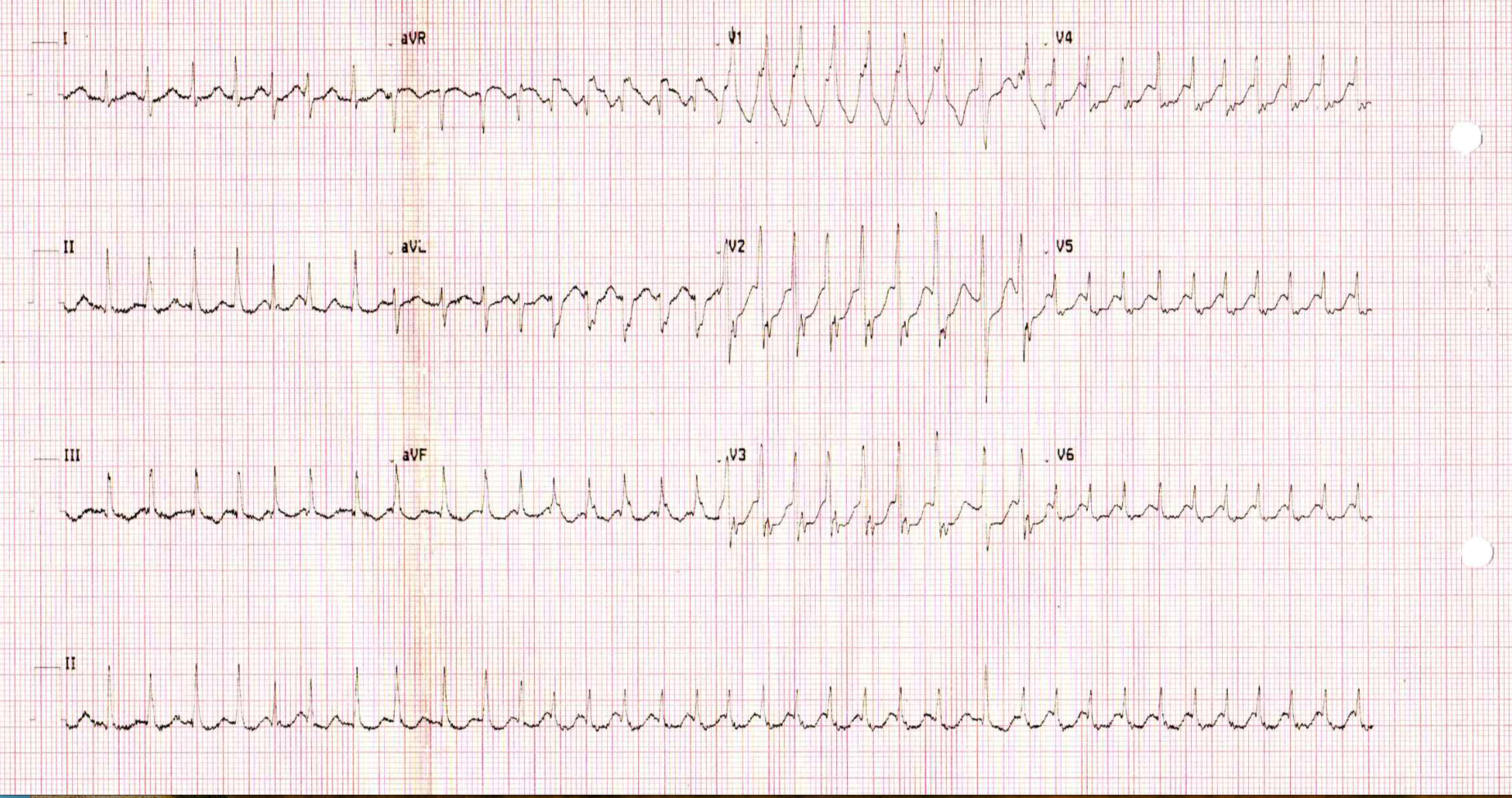
An anxious patient, as the palpitations were not self-limited and the irregular narrow QRS
tachycardia persisted, amiodarone was indicated with a 300mg loading dose. and in infusion 600mg. After
2 hours of observation, Atrial Fibrillation persisted with high ventricular response Fig. 1, due to
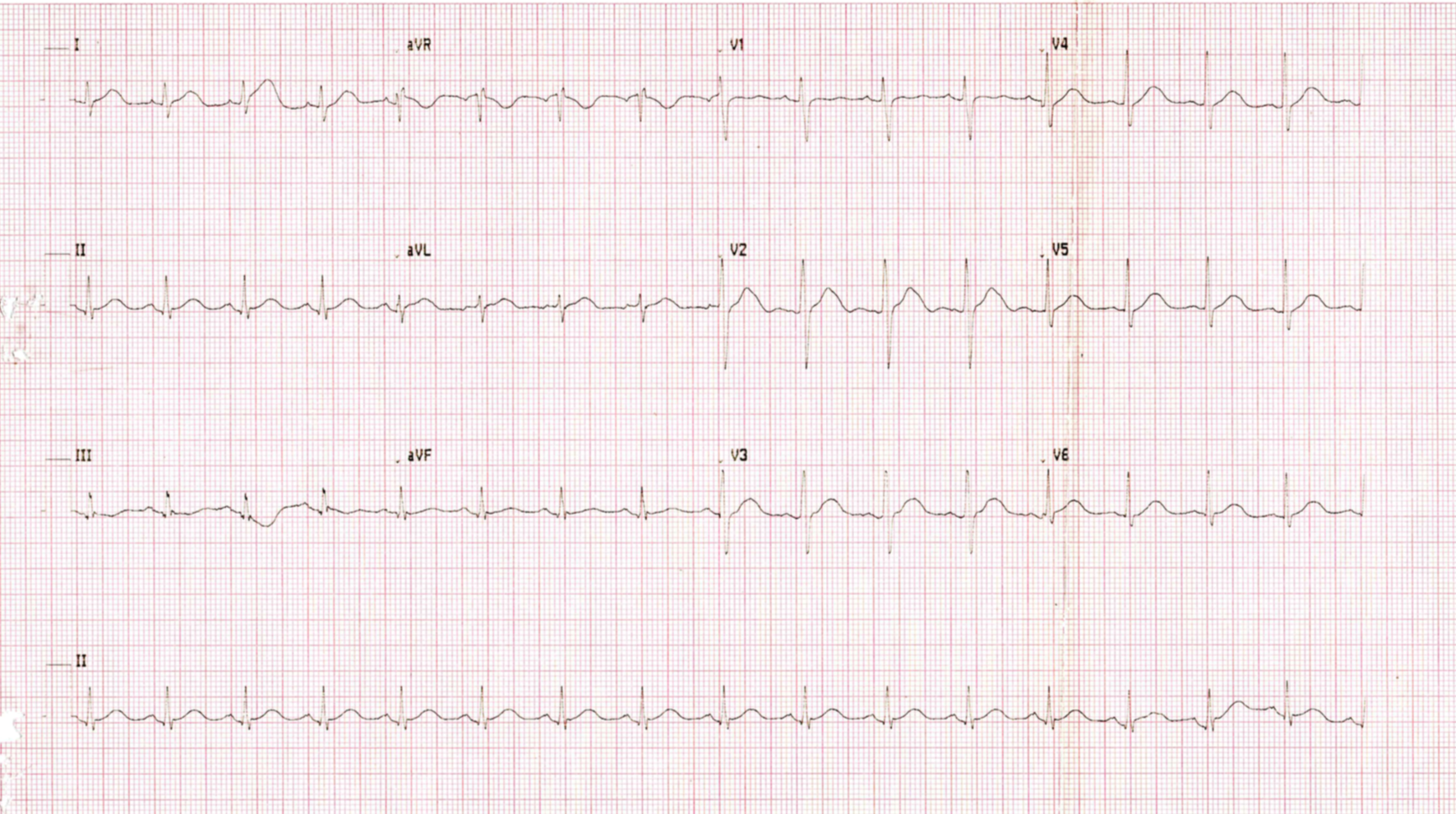
increased dyspnea and hemodynamic decompensation, it was decided to perform cardioversion under sedation
Fig. 2.
Electrical cardioversion vital functions Fc: 145 -160 x, ’PA: 80/60, SatO2 97%.
Propofol 1 mg /
kg was used as anesthetic, 150 joule was discharged, leaving sinus rhythm with the first discharge, the
patient remains in the recovery unit for three more hours and is discharged for control by the
cardiology office and treatment with propofenone 150mg c / 12 x 1 month.
Thus, care with effective electrical cardioversion is concluded. Procedure without
complications, anticoagulation was not indicated, due to a greater risk of immediate postoperative
bleeding, she was discharged home.
During the follow-up of the patient by telephone, at 24 and 48 hours postoperatively, the
patient remained asymptomatic, with no recurrence of arrhythmia.
At 6 months of evolution of the patient, he underwent laparoscopic cholecystectomy, under
balanced inhalation general anesthesia, without intercurrences, remaining in sinus rhythm.
|
|
DISCUSSION
Ambulatory surgical procedures are increasingly frequent in Peru, although there are very few
independent ambulatory surgery centers, this clinical case was presented in one of them. In recent
years, due to a marked development of surgeries and new techniques in anesthesia with ultra-short-acting
drugs, as well as an optimal perioperative evaluation and preparation of the patient, both for
anesthesia and for surgery. The improvements in the recovery unit have contributed to this being
possible, (1,2) however some procedures are complicated and
anesthesiologists must be attentive to these medical events, which may occur in the perioperative
period. It is very important to understand the mechanisms of AF by cardiologists, anesthesiologists and
surgeons, as well as the treatments to provide timely patient care.
The preoperative evaluation, checklist, signed informed consents, preoperative education were
completed. The technique used was intravenous at doses according to the monitoring of anesthetic depth,
with no intercurrences in the intraoperative period, however 30 'after arriving at the anesthetic
recovery unit, he presented tachycardia and later atrial fibrillation.
Postoperative atrial fibrillation (POAF), we wonder what the prevalence is in patients without a
history of AF, in outpatient procedures or non-cardiac surgeries. Koren O, et al.(3) carried out a descriptive study, which included 24,125 patients undergoing
non-cardiac surgery and found a prevalence of 2.69 x 1000 patients, more frequent in hip fixation and
abdominal surgeries. Bessissow A. et al(4)report an incidence of 3% in adult
patients for non-cardiac
surgeries, with electrical cardioversion being the most effective treatment to restore sinus rhythm with
a success rate of 69.2%(3).
The pathophysiology of AF in non-cardiac surgeries is not well understood, it is believed that
in most cases AF is caused by the combination of multiple mechanisms and factors, first the activation
of the sympathetic system, due to the stress of surgery and catecholamine release, other clinical
circumstances such as hypovolemia, intraoperative hypotension, anemia, trauma and pain, can affect
sympathetic activity and cause metabolic imbalances (hypoglycemia or electrolyte disturbances).
Hypoxia can also cause arrhythmia, due to vasoconstriction of the pulmonary vein and increased
pressure in the right ventricle. Likewise, hypervolemia could cause an increase in intravascular volume,
which causes a stretching of the right atrium.
Likewise, Bessissow A et al.(4) correlated the presence of arrhythmias
with elevated inflammatory markers, such as C-reactive protein (CRP), white blood cells, and
interleukins. In this case, apart from surgical stress, none of these factors were present, it was a
relatively bloodless surgery, in a young patient without major hemodynamic changes, according to the
registry, AF did not present intraoperatively either.
Parida S Et. Al.(5), make a review on tachyarrhythmias, explored a
temporal relationship between medications in the perioperative period, the mechanisms, as well as the
drugs that could trigger them, evaluated the factors and classified them according to the patient,
pathology, position, The pharmacology and the procedure, regarding the medications, mentions
inhalational anesthetics, atropine, spinal anesthesia and concludes that the choice of anesthetic agents
may be important to mitigate the incidence of tachyarrhythmias. However, none of the agents that the
authors mention as not recommended were used.
Kounis N et al.(6) conducted a review where it is mentioned that AF
affects 35 million people in the world annually, it is a common postoperative complication that can
occur spontaneously during general and local anesthesia.
The authors consider that the higher incidence of AF is correlated with the activation of the
autoimmune system, paroxysmal atrial fibrillation (AF) is the most common of arrhythmias, they occur in
3% of patients, many resolve spontaneously but if AF paroxysmal persists, the risk of stroke in one year
is 1.5%, compared to 0.3%, of those who do not have it. In addition, heart failure, myocardial
infarction, and cardiac arrest can occur in patients with paroxysmal AF.(7)
Therefore, the follow-up of these patients is very important to prevent later complications.
Likewise, in a systematic review,(8)whose main objective was to
identify the incidence of new-onset AF after general surgery, the secondary objective was to know the
risk factors and associated results (mortality and thromboembolic disease), not studied patients with a
history of AF. The incidence of postoperative AF was associated with chest and abdominal operations, as
well as a duration of more than 600 min. However, they suggest multicenter studies, in order to better
stratify risk factors.
We think, what could have triggered this atrial fibrillation, in terms of anesthesia the
intravenous technique was used.
There are many studies on the safety of this technique, among them, propofol and remifentanil
have very few arrhythmogenic properties, Propofol(9) does not alter HR, it
has
a small negative
chronotropic effect. Likewise, opioids reduce HR through a central mechanism that decreases sympathetic
tone and increases vagal tone.
The European Society of Cardiology, (10)classifies AF into 5 types:
recently
diagnosed without
previous history, paroxysmal that lasts less than 7 days with or without intervention, persistent that
lasts more than 7 days, long-term persistent that lasts more than one continuous year and the permanent
one that is accepted by the patient and the doctor and no further attempts will be made to restore or
maintain sinus rhythm.
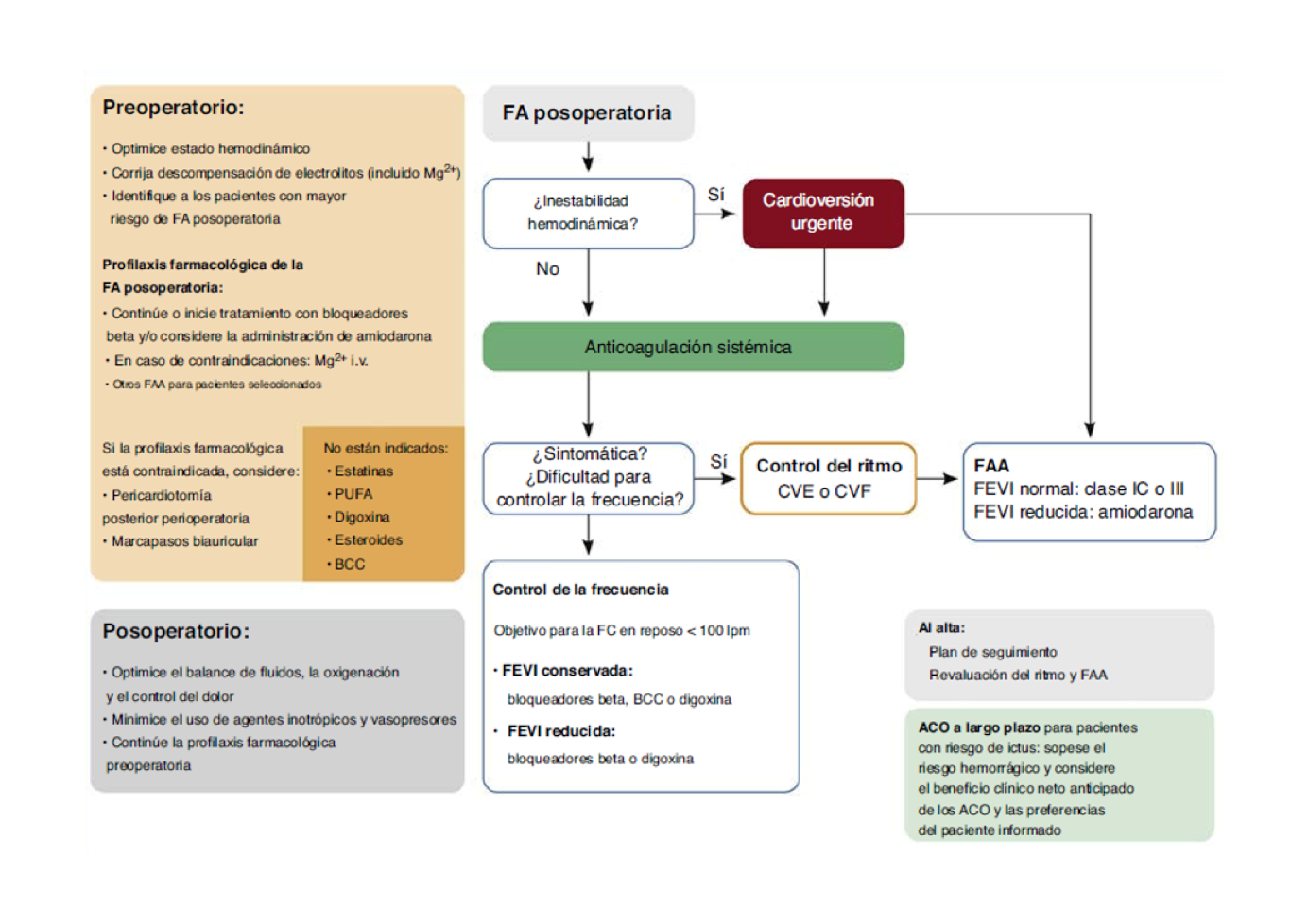
As recommended(10) (Fig. 3) the acute treatment
of FAPO. will depend
on the hemodynamic status. If we have signs of instability, such as hypotension, hypoperfusion,
sensorial disorder, among others, electrical cardioversion (ECV) will be performed.
If we have signs of hemodynamic stability and symptoms persist or we have difficulty controlling
the heart rate, we can choose a rhythm control strategy. This can be achieved by pharmacological
cardioversion with group I-C or III antiarrhythmic drugs or ECV. In the case described, an initial
attempt was made with amiodarone, in a loading dose followed by intravenous infusion and two hours
later, palpitations associated with dyspnea persisted and, as recommended by clinical practice
guidelines, ECV was performed effectively.
Cardiovascular events are the third most frequent problem in post-anesthesia care units(11).
It is concluded that perioperative AF does not induce any adverse heart disease such as
cardiogenic shock.(12)
The long-term prognosis is variable and the treatment options are diverse, from the simple
control of symptoms, to the most aggressive strategies, such as ablation with three-dimensional
electroanatomic mapping, which requires the identification of high-risk patients, who they will require
a more aggressive treatment, from the beginning of the evaluation of their FA(13).
If we speak in terms of primary prevention, we would consider a FAPO high risk, in terms of the
association with comorbidities and complications. Therefore, predicting the incidence of postoperative
AF would be useful for short- and long-term management, such as anticoagulation therapy.
|
CONCLUSION
In this case, despite the adequate patient selection, the surgical and anesthetic methods, the picture of POAF was presented, early diagnosis and timely treatment was made, with cardioversion due to hemodynamic instability, the patient was young, without significant medical history. The purpose of this review is to take into account a preventive and therapeutic approach, have a comprehensive vision in the treatment of AF, in outpatient surgery centers and provide our patients timely care.
Authors' contributions: The authors participated in the conception and design of the
project; collection, analysis and interpretation of the results; writing, critical review and
approval of the final version of the article.
Financing: Self-financed
Conflict of Interest: The authors declare that they have no conflict of interest.
Received: June 17, 2021
Approved: July 24, 2021
Correspondence: Miryam Céspedes Morón
Address: Calle Murillo 281 Dpto. 203 San Borja
Phone: 998703847
Email: miryamc18@hotmail.com
REFERENCES
