CASO CLÍNICO
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2022 - Universidad Ricardo Palma10.25176/RFMH.v22i2.4397
PÁNCREAS ECTÓPICO INCIDENTAL EN VESÍCULA BILIAR: REPORTE DE CASO
INCIDENTAL ECTOPIC PANCREAS IN GALLBLADDER: A CASE REPORT
Pedro Zamora-G1,a, Carmen Yagui-U2,b, José Somocurcio-P1,b, Ronald Goicochea-A1,c
1 Hospital Nacional Edgardo Rebagliati Martins, Lima, Perú.
2 Hospital Nacional Daniel A. Carrión, Callao, Perú.
a Mg, MD Especialista en Cirugía general.
b Mg, MD Especialista en patología clínica.
c MD, Especialista en cirugía general.
ABSTRACT
Ectopic pancreas in the gallbladder is a rare finding, with an incidence of less than 0.5% of the cases described in the literature. We report the case of a 26-year-old woman who went to the emergency room for abdominal pain and underwent laparoscopic cholecystectomy. The pathology report described ectopic pancreatic tissue in the gallbladder wall. This finding must be thoroughly evaluated due to the susceptibility of pancreatic tissue to pathologies such as pancreatitis, cystic lesions, and malignant degeneration. It must be considered in the context of a gallbladder polyp associated with digestive symptoms.
Keywords: Gallbladder; pancreas; ectopic tissue; incidental findings. (Source : MeSH - NLM).
RESUMEN
El páncreas ectópico en vesícula biliar es un hallazgo poco frecuente, con una incidencia menor a 0.5% de los casos descritos en la literatura. Reportamos el caso de una mujer de 26 años que acude a emergencia por dolor abdominal quien fue sometida a una colecistectomía laparoscópica. El reporte anatomopatológico describió tejido pancreático ectópico en la pared de la vesícula biliar. Este hallazgo debe ser evaluado minuciosamente debido a la susceptibilidad del tejido pancreático a patologías como pancreatitis, lesiones quísticas y degeneración maligna, y debe ser considerado en el contexto de un pólipo vesicular asociado a sintomatología digestiva.
Palabras Clave: Vesícula biliar; páncreas; tejido ectópico; hallazgo incidental. (Fuente: DeCS BIREME).
INTRODUCTION
Pancreatic ectopia is the nding of normal pancreatic tissue in an abnormal location (1). The most common presentation sites are the stomach, duodenum, and small intestine (1-3), with gallbladder location being infrequent (2,3). The incidence of pancreatic tissue in the gallbladder is usually less than 0.5% reported in all cases of the ectopic pancreas(3). These cases are usually asymptomatic (1,4-5); however, they may be associated with abdominal pain, nausea, and anorexia(3). This ectopic pancreatic tissue can degenerate into metaplasia or malignant neoplasia, which is why its diagnosis and treatment are important (1). We report the incidental nding of ectopic pancreatic tissue in the fundus of a gallbladder in a patient operated on for gallbladder polyp associated with symptoms.
CASE REPORT
A 26-year-old female patient with no relevant medical history attends the emergency room of a local
clinic for evaluation of abdominal pain associated with vomiting and liquid stools. This condition began
two days ago. She is evaluated in an emergency by the doctor on duty who ordered auxiliary tests (blood
count and electrolytes); the results were leukocytes at 8.12 103/uL hemoglobin 12.7g/dL platelets 254
103/uL Na+ 137.6 mmol/L K+ 3.82 mmol/L Cl- 105 mmol/L; the patient was discharged with proton pump
inhibitors and antispasmodics.
The patient was readmitted to the emergency department two days later due
to abdominal pain associated with general malaise and nausea. The general surgeon evaluates the patient
and indicates additional tests (blood count and urine test) and abdominal ultrasound. Laboratory tests
remained within normal values , and abdominal ultrasound only incidentally revealed a 7mm polyp in the
gallbladder. The patient was discharged with an indication for evaluation in the general surgery
outpatient clinic and possibles cheduling for elective surgery (cholecystectomy). Five days later, the
patient was readmitted for the third time to the emergency department due to abdominal pain that
radiated to the right dorsal region, associated with nausea, vomiting, and a sensation of temperature
rise. The general surgeon reassessed the patient and requested another abdominal ultrasound for acute
cholecystitis.
Ultrasound does not show inflammatory gallbladder changes; however, a 7mm gallbladder polyp is
described; therefore, she is discharged with an indication of evaluation by external consultation. The
patient is evaluated by a general surgery outpatient clinic and scheduled for elective surgery
(laparoscopic cholecystectomy), which is performed 10 days after the first emergency admission. The
surgical procedure (laparoscopic cholecystectomy) was performed without complications. The patient
evolved favorably and was discharged on the second postoperative. The patient is evaluated by an
outpatient clinic 10 days after discharge, without presenting any symptoms.
The anatomopathological examination of the gallbladder revealed in macroscopy a gallbladder of
4.5x2x1.5cm, partially covered by smooth grayishgreen serosa. On cutting the middle wall 0.2cm thick, 2
yellowish polyps of 0.2 and 0.1cm were identied, and, in addition, to the presence of 1 grayish nodule
in the distal third of 0.9cm. Microscopic evaluation revealed chronic cholecystitis with inflammatory
polyps and ectopic pancreas in the distal wall of the gallbladder (Figure 1A-B).
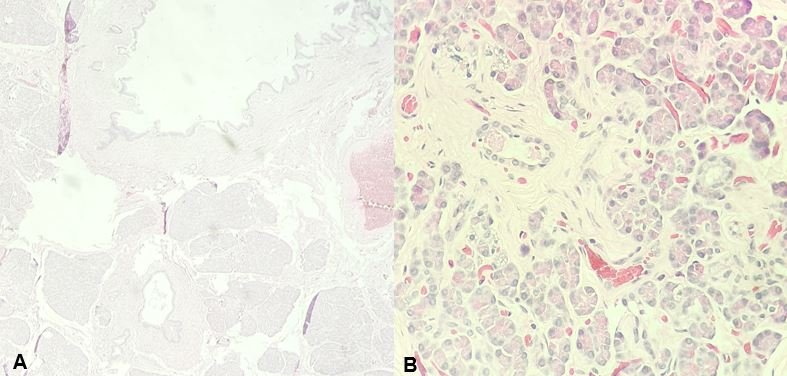
A: The wall with the presence of ectopic pancreatic tissue at the muscle layer level (Hematoxylin-Eosin staining x4).
B: Ectopic pancreatic tissue (Hematoxylin-Eosin staining x40).
DISCUSSION
A choristoma (normal ectopic tissue located in an abnormal location) in the form of an ectopic or
heterotopic pancreas is an embryological abnormality defined as pancreatic tissue with an aberrant
location without presenting anatomical, vascular or neural connection to the pancreas (1). The most common location of the ectopic pancreas in the upper digestive
tract (stomach, duodenum, jejunum, or spleen) (1-3) ; however,
it is rarely found elsewhere such as the ileum, mesentery, lungs, gallbladder, liver, bile duct, bile
ducts, Meckel's diverticulum, or mediastinum (2,3) . The first
description of the ectopic pancreas in the gallbladder dates back to 1916, by Otschkin (1) , and to date, approximately 40 cases have been described worldwide
(1-3).
The particular case of ectopic pancreatic tissue in the gallbladder is extremely rare and is
usually diagnosed when performing the examination. Pathology of a gallbladder that was removed during
cholecystectomy for symptomatic gallbladder disease (2) . Preoperative
diagnosis is practically impossible and, in general, this condition is found incidentally during
necropsies or laparotomies for other reasons (1,2) . During
reviews carried out in other countries, the ectopic pancreas in the gallbladder had an incidence of less
than 0.5%(3).
Epidemiologically, the ectopic pancreas can present at any age, but it is frequent between the
fourth and sixth decades of life, being more frequent in males (three to five times more); however, if
the ectopic pancreas is found in the gallbladder, the patient is usually a woman, since statistically
surgical gallbladder pathology is more common in women than men (1).
The most accepted theory of the formation of this ectopic tissue is the one that describes a
separation during the rotation of the gastrointestinal tract in the embryonic period (1). However, other reviews indicate an alteration in the Notch signaling
system, which leads to differentiation during the development of the endoderm of the foregut; however,
no theory explains this alteration exactly (2).
The symptomatology of the ectopic pancreas is not specific, which include upper abdominal pain,
anorexia, postprandial vomiting and weight loss (3) ; however, most cases are
asymptomatic (1,4,5). Other reviews indicate
tumors with mass effect up to perforation, gastrointestinal bleeding, and abdominal distention,
depending on location in the gastrointestinal tract (4). These ectopic tissues
can lead to the development of metaplasias or neoplasias that can affect the normal pancreas; however,
the finding of these tissues still lacks clinical significance and requires an exhaustive pathological
examination to establish the diagnosis (1,6) Being normal
pancreatic tissue lodged in another location can be susceptible to pathologies typical of pancreatic
tissue in a normal location, such as acute and chronic pancreatitis, formation of cystic lesions,
pseudocysts, calcifications, pancreatic cancer, and endocrine tumors (1).
Regarding diagnosis, even though it has already been mentioned that preoperative diagnosis is usually
very difficult and is usually found incidentally when this pathology is found in an area of the
digestive tract such as the stomach, duodenum, or small intestine, it is usually associated with
digestive bleeding; Therefore, a fine-needle biopsy of the lesion by ultrasound endoscopy is a tool
widely used by gastroenterologists to define the diagnosis and potential treatment (6). In the present case, the ectopic pancreatic tissue was found in the
gallbladder, which made the preoperative diagnosis difficult and was performed by pathological
examination incidentally.
The classification of the ectopic pancreas was described by Von Heinrich and later modified by
Gaspar Fuentes, in which he describes 4 types(1,3) : Type 1:
the presence of pancreatic acini, ducts, and islet-like glands, Type 2: canalicular variant with ducts
pancreatic, Type 3: exocrine pancreas with acinar tissue, not endocrine tissue. Type 4: Endocrine
pancreas with islet cells, not exocrine tissue. The usual size is small and usually does not exceed 2 or
3 cm; likewise, it usually lodges in the peri-vesicular fatty tissue(3,6). In other cases, they can simulate a polypoid lesion and vary from
millimeters to 4cm; 50% of the lesions originate in the gallbladder neck and are present in the
submucosa(1,2).
Being normal pancreatic tissue lodged in another location can be susceptible to pathologies
typical of pancreatic tissue in a normal location, such as acute and chronic pancreatitis, formation of
cystic lesions, pseudocysts, calcifications, pancreatic cancer, and endocrine tumors (1). Regarding diagnosis, even though it has already been mentioned that
preoperative diagnosis is usually very difficult and is usually found incidentally when this pathology
is found in an area of the digestive tract such as the stomach, duodenum, or small intestine, it is
usually associated with digestive bleeding; Therefore, a fine-needle biopsy of the lesion by ultrasound
endoscopy is a tool widely used by gastroenterologists to define the diagnosis and potential treatment
(6). In the present case, the ectopic pancreatic tissue was found in the
gallbladder, which made the preoperative diagnosis difficult and was performed by pathological
examination incidentally.
The ectopic pancreas in the gallbladder is a fairly rare and infrequent pathology that presents a challenge for clinical and surgical medical personnel. Due to the potential for real malignancy that it may represent, the diagnosis should not be underestimated by medical personnel and should be considered as a differential diagnosis in the context of gallbladder polyps associated with upper gastrointestinal symptoms. Likewise, it requires meticulous work by the pathologist for an adequate evaluation of the surgical specimen.
Authorship contributions: The authors participated in the genesis of the idea, project
design, data collection and interpretation, results analysis and manuscript preparation of this
research work.
Funding sources: Financing.
Conflicts of Interest: The authors express that there are no conicts of interest when writing the manuscript.
Received: December 06, 2021
Approved: February 09, 2022
Correspondence: Ronald Alberto Goicochea Arevalo
Address: Jiron Joaquin Bernal 595 – Dpto 701. Lince – Lima – Peru.
Telephone number: 945 666 530
E-mail: ronald_goicochea@hotmail.com
REFERENCES
