ARTICULO ORIGINAL
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2022 - Universidad Ricardo Palma10.25176/RFMH.v22i3.4753
GAPS IN ACCESS TO ONCOLOGICAL TREATMENT IN A REFERENCE HEALTH HOSPITAL IN THE SOUTH OF LIMA IN THE YEAR 2019
BRECHAS DE ACCESO AL TRATAMIENTO ONCOLÓGICO EN UN HOSPITAL DE SALUD DE REFERENCIA DEL SUR DE LIMA EN EL AÑO 2019
Reina Bustamante-Coronado1,2,a, José M. Vela- Ruiz2,b, Omar Paredes-Olivares3, Ricardo A. Carreño-Escobedo1,c
1Scientific University of the South, Lima, Peru.
2Hospital María Auxiliadora Oncology Research Unit. Lima Peru.
3Peruvian League Fight against cancer.
aSpecialist in Breast, Skin and Soft Tissue Surgical Oncology
bMaster in Management and Health Services.
cDoctor in Medicine
ABSTRACT
Introduction: Cancer, a chronic disease that has a high incidence with 14.1 million people and more than 8.1 million deaths, generating a large access gap according to the user's perception. Objectives: To determine the gaps in access to cancer treatment in a Hospital in Peru in 2019, due to predisposing, enabling and necessary factors. Method: observational, descriptive, cross-sectional study with 185 patients diagnosed with cancer who were treated at the oncology department of the Hospital María Auxiliadora between March and December 2019, applying a random survey. Results: The predisposing factors for the gap in access to cancer care were: primary education or none (p< 0,001), female gender (p=0.043), being afraid of a cancer diagnosis (p=0.000), being afraid of interventions (p=0.043) and being over 65 years old (p=0.000), having feelings of helplessness (p=0.000). Within the enabling factors as a gap: not having a job (p=0.011), payment for exams in a private way (p=0.035), stop working (p=0.039), payment for medicines in a private way (p= 0.000), resort to the loan (p= 0.009), health expenditure between 501-1000 soles in health (p=0.048). Of the necessary factors: having moderate to severe anemia (p=0.002) or having required more than one treatment in combination (p=0.003). Conclusions: there is a gap for cancer care such as those concerning the predisposing factor (fear of cancer diagnosis and treatment); enabling (infrastructure and equipment, payment for medicines) and necessary factor (severe anemia).
Keywords:Cancer care facilities; Healthcare disparities; Medical Oncology. (fuente: MeSH NLM).
RESUMEN
Introduction: EL cáncer, enfermedad crónica que presenta alta incidencia con 14,1 millones de personas y más 8,1 millones de mortalidad, generando una gran brecha de acceso según la percepción del usuario. Objetivos: Determinar las brechas de acceso al tratamiento oncológico en un Hospital de Perú en el año 2019, por factores predisponentes, habilitantes y necesarios. Método: estudio observacional, descriptivo, transversal con 185 pacientes con diagnóstico de cáncer que se atendieron en el departamento de oncología del Hospital María Auxiliadora entre marzo y diciembre 2019, aplicando una encuesta aleatoria. Resultados: Los factores predisponentes de brecha para acceso de atención oncológica fueron: escolaridad primaria o ninguna (p=0,000), sexo femenino (p=0,043), tener miedo al diagnóstico de cáncer (p=0,000), tener miedo a las intervenciones (p=0,043) y ser mayor de 65 años (p=0,000), tener sentimientos de impotencia (p=0,000). Dentro de los factores habilitantes como brecha: no tener trabajo (p=0,011), pago por exámenes en forma particular (p= 0,035), dejar de trabajar (p= 0,039), pago por medicamentos en forma particular (p=0,000), recurrir al préstamo (p=0,009), gasto en salud entre 501-1000 soles en salud (p=0,048). De los factores necesarios: tener anemia moderada a severa (p=0,002), haber requerido más de un tratamiento en combinación) (p=0,003). Conclusiones: existe una brecha para la atención oncológica como aquellas concernientes al factor predisponente (miedo al diagnóstico y tratamiento oncológico); habilitantes (infraestructura y equipamiento, pago por medicamentos) y necesarios (anemia severa).
Palabras Clave:Instituciones oncológicas; Disparidades en atención de salud; Oncología Médica. (Source: DeCS BIREME).
INTRODUCCIÓN
Cancer is a chronic disease with a high incidence with more than 14.1 million people diagnosed and more than 8.1 million dying annually globally(1), being the countries with low and middle incomes such as Latin America and Peru among them the ones that are most affected by the high burden of disease that it causes in the population, being that the mortality reported in Peru in recent years is 122 per 100,000 inhabitants (2,3).
A characteristic of low- and middle-income economies is the existing limitation to the diagnostic process and treatment of the heterogeneous group of diseases grouped as cancer, causing a decrease in the opportunity for cure or prolongation of life (2). High-income countries have a high incidence, but mortality is lower due to early diagnosis and updated treatments. In low- and middle-income countries, there is a high incidence and high mortality; for example, cancer of the cervix or liver predominates in countries with a low human development index, which is linked to infections. Therefore, the implementation of primary prevention strategies through vaccination against the human papillomavirus, and hepatitis, is a key piece to reducing the risks of contracting them, imitating developed countries (4).
In the process of carcinogenesis and disease development, it is imperative to have diagnostic processes, which, given their complexity, are carried out in hospitals that have all the infrastructure, specialized human resources, and a guarantee that financing is not a barrier to receiving treatment. the corresponding treatment according to the stage (5,6).
Concerning access to health care, the ability of a group of people or an individual to seek and obtain such care (7) ; there are many gaps for cancer care, which may depend on the individual himself related to their fears, beliefs, taboos they have about the disease; at the educational level, gaps related to aspects that involve financing, regarding social aspects, the organization of services, and the effects of treatments on the individual (8). Various international studies report access gaps, grouping them into geographic, administrative, economic, and socio-cultural (9,10,11,12,13). These access gaps are found throughout the cancer care process, from screening to treatment and palliative care (10) Patients are treated in advanced stages, such as in Peru, where approximately 80% of patients arrive in stage IV (3) causing high mortality.
Barriers to access to health care have been studied in various contexts such as Latin America, Asia, North America, and Europe, to better understand the phenomenon (12,14,13,15), showever little is known about the barriers faced by our patients who come to the referential hospital in the south of Lima in Peru in search of cancer care.
The results of this study can help regulatory and care systems to understand the factors that hinder health care in cancer cases so that they can be corrected.
The objective of the study was to determine the gaps in access to cancer treatment at the María Auxiliadora Hospital (HMA), Lima, Peru.
METHODOLOGY
Design and study area
The present study is of an observational, descriptive, cross-sectional type, carried out in the oncology care environments of the Oncology Department of the María Auxiliadora Hospital, located in the city of Lima-Peru, from March to December of 2019.
Population and sample
The sample size was made based on a population of 300 patients diagnosed with cancer (average number of new patients per year according to HIS-MINSA data, attended in the department's outpatient clinic according to the Statistics Office). For the selection of the sample, a random probabilistic sampling (simple random) was carried out. The patient was given a piece of paper extracted from a sealed envelope where 300 annotations were included. The one who obtained the annotation "INCLUDED" participated in the study, not considering quota by sex, obtaining a sample of 185 patients of both sexes, who signed informed consent. The randomly selected patients all had a Comprehensive Health System (SIS).
The inclusion criteria of the work were outpatients with a histopathological diagnosis within the first 10 most frequent cancers (prostate, breast, cervix, gastric, lymphoma cancer). Patients under 18 years of age and those patients who did not have the psychic competence to consent to their participation in the study, as well as those who had difficulty understanding and answering the survey questions for data collection, were excluded. For this type of study, the degree of cancer or stage was not considered on this occasion because it was not a study that evaluated survival, but rather a perception of care, which we consider to be a gap or barrier to care.
Variables and instruments
To carry out the study of gaps in access to treatment in the María Auxiliadora hospital oncology department, we used Ronald Andersen's behavioral model (8) on the use of health services, where the following factors are considered: predisposing, enabling and necessary factors.
The predisposing factors are composed of the following ten demographic indicators: age; sex; scholarship; occupation; family composition; myths, beliefs, and taboos around cancer; fear of diagnosis; fear of surgical interventions; feelings of helplessness and shame to show the body at the time of clinical examination.
Within the indicators in the enabling factors, we have those related to financing such as economic condition, spending, and health insurance, enabling factors related to an organization such as infrastructure in the oncology area, the number of beds in hospitalization, size of the clinics, distribution of hospitalization, specialized human resources, equipment, service hours, waiting time for care since symptoms presented, waiting time for care in the oncology service, time used to get to the oncology service, time to use the different services in your care.
Among the necessary factors we have: aspects related to the person in the psychic aspect such as feelings about the disease, knowledge of the disease, feelings about the care received, physical aspects such as the functional status of the patient, clinical status, type of treatment, weight, height, hemoglobin (factors related to the physical condition of the person). To consider anemia was considered as mentioned by Van Belle (16) , where these values are considered prognostic regardless of the type of neoplasm or sex.
The questionnaire was submitted to an expert judgment made up of 1 gynecologist, 2 surgical oncologists, 1 medical oncologist, and 1 medical oncologist dedicated to the part of palliative care approved in the thesis project presented to the ethics committee of the Universidad Científica del Sur with the registration code 321-2018-POS15.
Procedures
The questionnaire was applied to patients in chemotherapy settings and oncology medicine and oncology surgery clinics.
Statistical analysis
The analysis plan was carried out by entering the information into an Excel program from the original form approved by expert judgment. Then, the analysis of the information was carried out in the statistical package SPSS version 21.
A descriptive analysis of the gaps in access to oncology services by enabling, predisposing and necessary factors was carried out. The variables in the qualitative measurement scale were described with absolute and relative frequencies. The relationship between categorical variables has been compared using chi-square considering p<0.05 as a significant value.
For inferential analysis: Pearson's Chi-square value was calculated using the SPSS 21 statistical package, for 2 by 2 matrices (presence/absence of limiting factors), p<0.005 was considered significant.
Ethical aspects
Authorization was obtained from the head of the oncology department of the María Auxiliadora Hospital and the ethics committee of the Universidad Científica del Sur with registration code 321-2018-POS15 to develop the following study, identity confidentiality was guaranteed of the participants, as well as the informed consent of participation was obtained.
RESULTS
Table 1. The descriptive characteristics of the variables are described in Table 2.
Table 1. Diagnosis of cancer and sex
| tipo de cáncer o topografía | Sex | Total | |
|---|---|---|---|
| Female | Male | ||
| Breast cancer | 67 (49%) | 0 | 67 (36%) |
| Digestive tumors | 20 (15%) | 18 (37%) | 38 (21%) |
| Gynecological cancer | 36 (26%) | 0 | 36 (19%) |
| Urological tumors | 0 | 17 (35%) | 17 (9%) |
| Hematological neoplasms | 11 (8%) | 6 (12%) | 17 (9%) |
| Lung cancer | 1 (1%) | 6 (12%) | 7 (4%) |
| Metastatic cancer | 1 (1%) | 2 (4%) | 3 (2%) |
| Total | 136 (100%) | 49 (100%) | 185 (100%) |
Table 2. Descriptive variables of the sample.
| Hemoglobin | Frequency | Percentage |
|---|---|---|
| Normal (>11) | 78 | 42% |
| Mild (9-11) | 56 | 30% |
| Moderate (7-9) | 38 | 21% |
| Severe (<7) | 13 | 7% |
| Height | Frequency | Percentage |
| 1.5 metros or less | 36 | 19% |
| Between 1.51 and 1.60 meters | 139 | 75% |
| Greater than a 1.70 meters | 10 | 5% |
| Weight | Frequency | Percentage |
| Less than 50 kilos | 38 | 21% |
| Between 50 and 69 kilos | 107 | 58% |
| Greater than 70 kilos | 40 | 22% |
| Type of treatment received | Frequency | Percentage |
| Surgery | 54 | 29% |
| Chemotherapy | 80 | 43% |
| Radiotherapy | 29 | 16% |
| More than one treatment | 22 | 12% |
| Perception of the quality of care in Oncology Medicine | Frequency | Percentage |
| Very good care | 91 | 49% |
| Good care | 80 | 43% |
| Regular care | 13 | 7% |
| Poor care | 1 | 1% |
| Economic coping due to disease | Frequency | Percentage |
| Family savings | 92 | 50% |
| Two or more activities* | 42 | 23% |
| Pro-fund activities | 36 | 19% |
| Loan* | 13 | 7% |
| Sale of goods* | 2 | 1% |
| Payment for medications | Frequency | Percentage |
| If paid for medications | 113 | 61% |
| Did not pay for medications | 72 | 39% |
| Payment for exams | Frequency | Percentage |
| Did not pay for exam | 130 | 70% |
| If paid for exams | 55 | 30% |
| Working | Frequency | Percentage |
| If stopped working | 126 | 68% |
| Did not stop working | 4 | 2% |
| Did not have a job | 55 | 30% |
| Income | Frequency | Percentage |
| Less than 950 Soles | 3 | 2% |
| From 951 to 1200 Soles | 46 | 25% |
| From 1201 to 1400 Soles | 83 | 45% |
| From 1401 to 1600 Soles | 51 | 28% |
| From 1601 to 1800 Soles | 2 | 1% |
| Has a job | Frequency | Percentage |
| If has a job | 130 | 70% |
| Does not have a job | 55 | 30% |
| Fear of diagnosis | Frequency | Percentage |
| Yes, afraid of diagnosis | 117 | 63% |
| Not afraid of diagnosis | 68 | 37% |
| Schooling | Frequency | Percentage |
| None | 12 | 6% |
| Incomplete primary school | 29 | 16% |
| Complete primary school | 21 | 11% |
| Incomplete secondary school | 25 | 14% |
| Complete secondary school | 65 | 35% |
| Technical or professional | 33 | 18% |
| Occupation | Frequency | Percentage |
| Does not declare an occupation | 82 | 44% |
| Technician | 79 | 43% |
| Professional | 24 | 13% |
| Race | Frequency | Percentage |
| Mestizo | 173 | 94% |
| White | 9 | 5% |
| Mulatto | 3 | 1% |
| Sex | Frequency | Percentage |
| Female | 136 | 74% |
| Male | 49 | 26% |
| Age | Frequency | Percentage |
| From 18 a 40 years | 37 | 20% |
| From 41 to 65 years | 109 | 59% |
| Over 65 years old | 39 | 21% |
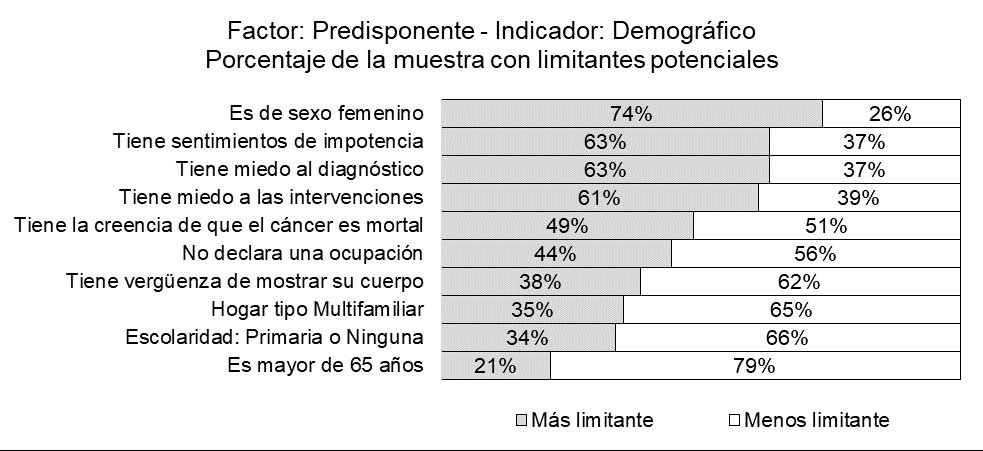
The gaps in access to cancer treatment due to demographic predisposing factors that affect more than 50% of the patients of the María Auxiliadora Hospital for the year 2019 were: Being female, having feelings of helplessness , being afraid of diagnosis and being afraid of interventions (Figure 1).
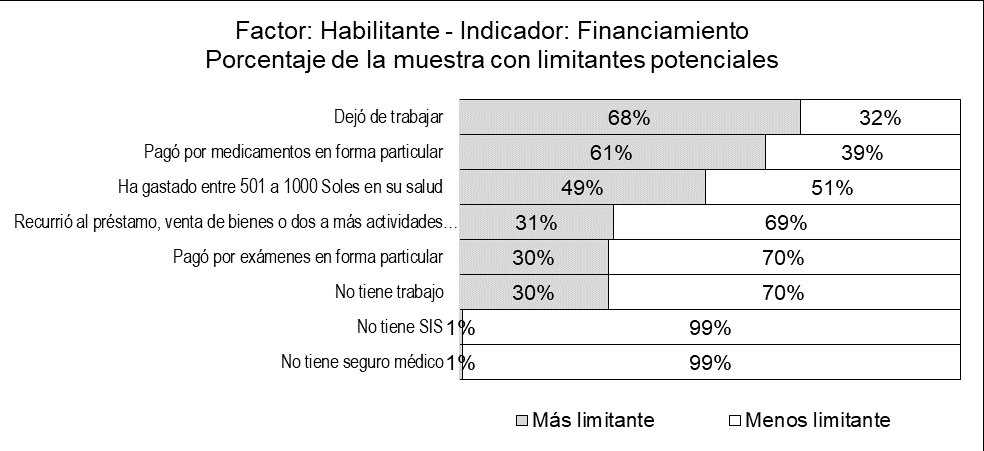
The gaps in access to cancer treatment due to enabling factors related to financing that affect more than 50% of the patients of the María Auxiliadora Hospital for the year 2019 were: Losing their job and having to pay for their medications in a particular way (Figure 2).
The gaps in access to cancer treatment due to enabling factors related to the organization that affects more than 50% of the patients of the María Auxiliadora Hospital for the year 2019 were: Having a poor knowledge of the diagnostic imaging services available in the HMA, waiting more than 24 weeks from the onset of their symptoms to being treated at a health facility, not finding medications available in the HMA pharmacy and having treated the symptoms of their illness in a health center (with less resolution capacity than a hospital ) (Figure 3).

The gaps in access to cancer treatment due to necessary factors related to the perception of their own needs that affect more than 50% of the patients of the María Auxiliadora Hospital for the year 2019 were: Being very/very afraid of cancer (Figure 4).

To extend the statistical analysis, an analysis was carried out for 2 by 2 matrices using the presence and absence of limiting factors, crossing the following factors: predisposing, enabling, and necessary factors, considered significant p<0.005. The predisposing factors that cause a gap in cancer care were found mainly: being afraid of diagnosis (p=0.000), having feelings of helplessness (p=0.000), being ashamed to show the body at the time of the clinical examination (p=0.003), being female (p=0.043), being over 65 years old (p:0.000), primary education or none (p=0.000). The enabling factors that cause the oncology care gap were found mainly: There was no availability of medications (p=0.000), he paid for tests in a private way (p=0.035), it has taken more than 60 minutes to be seen in the Oncology office ( p=0.011), waited more than 24 weeks from the onset of their symptoms to go to the health facility (p=0.031), it is difficult to get an oncology appointment (p=0.039), they only know that the HMA has an ultrasound machine (p= 0.048), has spent between 501 and 1000 soles on his health (p=0.048), does not have a job (p=0.031), did not deliver the results of the laboratory tests on time (p=0.023), does not have a job (p =0.031).
Within the enabling factors, the following indicators behave as an access gap: not having a job (p=0.011), paying for exams in a private way (p=0.035), stopping working (p=0.039), paid for medicines in a private way (p=0.000), sale of goods or carry out two or more activities to finance the treatment, health expenditure between 501-1000 soles in health (p=0.048), resorted to the loan, sale of goods, two or more activities to finance their treatment (p=0.045). Among the necessary factors that have behaved as an access gap are mainly: having moderate to severe anemia (p=0.002), have required more than one combined treatment (surgery, radiotherapy, chemotherapy) (p=0.003), their main cancer information provider is not a doctor (p=0.032), is shorter than 1.5 meters (p=0.020) (Table 3).
Table 3. Relationship between limiting factors.
| Indicator | Factors | Patients | % | Pearson's chi-square<0,05 | Bilateral significance |
|---|---|---|---|---|---|
| Demographics | Is older than 65 years | 39 | 100% | ||
| Demographic | Education: Primary or None | 29 | 74% | 37.001 | 0.000 |
| Financing | Does not have a job | 21 | 54% | 13.758 | 0.000 |
| Demogaphic | Is female | 136 | 100% | ||
| Perception | less than 1.5 meters tall | 32 | 24% | 5.427 | 0.020 |
| Financing | He does not have a job | 46 | 34% | 4.119 | 0.042 |
| Demographic | He is afraid of interventions | 89 | 65% | 4.016 | 0.043 |
| Demographic | Does not declare an occupation | 82 | 100% | ||
| Demographic | Schooling: Primary or None | 34 | 41% | 4.178 | 0.041 |
| Demographic | Schooling: Primary or None | 62 | 100% | ||
| Demographic | Is over 65 years old | 29 | 47% | 37.001 | 0.000 |
| Financiamiento | Does not have a job | 28 | 45% | 10.63 | 0.001 |
| Perception | Has moderate or severe anemia | 26 | 42% | 9.641 | 0.002 |
| Demographic | Does not declare an occupation | 34 | 55% | 4.178 | 0.041 |
| Demographic | Multifamily | 65 | 100% | ||
| PPerception | Has required more than one treatment in combination (Surgery, Chemotherapy or Radiotherapy) | 12 | 18% | 4.128 | 0.042 |
| Demographic | Fear of diagnosis | 117 | 100% | ||
| Demographic | He is afraid of interventions | 97 | 83% | 63.78 | 0.000 |
| Demographic | He has feelings of powerlessness | 86 | 74% | 14.417 | 0.000 |
| Demographic | He is ashamed to show his body | 53 | 45% | 6.447 | 0.011 |
| Financing | He paid for exams privately | 41 | 35% | 4.301 | 0.038 |
| Demographic | He is afraid of interventions | 113 | 100% | ||
| Demographic | Fear of diagnosis | 97 | 86% | 63.78 | 0.000 |
| Demographic | Has feelings of helplessness | 85 | 75% | 17.92 | 0.000 |
| Demographic | is ashamed to show her body | 53 | 47% | 8.921 | 0.003 |
| Demographic | Is female | 89 | 79% | 4.106 | 0.043 |
| Demographic | Has feelings of helplessness | 117 | 100% | ||
| Demographic | He is afraid of interventions | 85 | 73% | 17.92 | 0.000 |
| Demographic | He is afraid of diagnosis | 86 | 74% | 14.417 | 0.000 |
| Demographic | He is ashamed to show his body | 55 | 47% | 10.025 | 0.002 |
| Demographic | He is ashamed to show his body | 71 | 100% | ||
| Demographic | Has feelings of helplessness | 55 | 77% | 10.025 | 0.002 |
| Demographic | Has fear of interventions | 53 | 75% | 8.921 | 0.003 |
| Demographic | Has fear of diagnosis | 53 | 75% | 6.447 | 0.011 |
| Financing | resorted to loans, sale of goods or two or more activities to finance treatment | 28 | 39% | 4.021 | 0.045 |
| Financing | Does not have a job | 55 | 100% | ||
| Demographic | Is over 65 years old | 21 | 38% | 13.758 | 0.000 |
| Demographic | Schooling: Primary or None | 28 | 51% | 10.63 | 0.001 |
| Organization | Has taken more than 60 minutes to be seen at the oncology clinic HMA | 35 | 64% | 6.536 | 0.011 |
| Organization | Waited more than 24 weeks from the onset of symptoms until going to the health facility | 39 | 71% | 4.649 | 0.031 |
| Perception | Your main cancer information provider is not a doctor | 33 | 60% | 4.434 | 0.035 |
| Demographic | Is female | 46 | 84% | 4.119 | 0.042 |
| Financing | You have spent between 501 to 1000 Soles in your health | 91 | 100% | ||
| Organization | Only knows that the HMA has an ultrasound scanner | 71 | 78% | 3.899 | 0.048 |
| Financing | Working r126 | 100% | |||
| Perception | Has required more than one treatment in combination (Surgery, Chemotherapy or Radiotherapy) | 21 | 17% | 8.597 | 0.003 |
| Organization | It is difficult to get an oncology appointment | 26 | 21% | 4.26 | 0.039 |
| Financing | He paid for tests privately | 55 | 100% | ||
| Organization | Medications were not available | 40 | 73% | 7.616 | 0.006 |
| Organization | Laboratory tests were performed outside the hospital | 23 | 42% | 6.641 | 0.010 |
| Financing | Paid for medications privately | 40 | 73% | 4.466 | 0.035 |
| Demographic | Fear of diagnosis | 41 | 75% | 4.301 | 0.038 |
| Organization | Is Difficult to get an oncology appointment | 14 | 25% | 4.245 | 0.039 |
| Financing | Paid for medications privately | 113 | 100% | ||
| Organization | Medications were not available | 90 | 80% | 59.27 | 0.000 |
| Financing | Paid for tests privately | 40 | 35% | 4.466 | 0.035 |
| Financing | Resorted to loans, sale of goods or two or more activities to finance treatment | 57 | 100% | ||
| Perception | He has moderate or severe anemia | 23 | 40% | 6.742 | 0.009 |
| Demographic | He is ashamed to show his body | 28 | 49% | 4.021 | 0.045 |
| Organization | It is difficult to get an oncology appointment | 31 | 100% | ||
| Organization | They did not deliver the results of the laboratory tests on time | 4 | 13% | 5.199 | 0.023 |
| Financing/strong> | Working | 26 | 84% | 4.26 | 0.039 |
| Financing | Paid for tests privately | 14 | 45% | 4.245 | 0.039 |
| Organization | Only knows that the HMA has an ultrasound | 132 | 100% | ||
| Organization | Waited more than 24 weeks from the onset of symptoms to go to the health facility | 87 | 66% | 9.301 | 0.002 |
| Organization | Has taken more than 60 minutes to be seen at the HMA oncology clinic | 72 | 55% | 5.289 | 0.021 |
| Financing | Has spent between 501 to 1000 Soles in your health | 71 | 54% | 3.899 | 0.048 |
| Organization | Waited more than 24 weeks from the start of your symptoms to go to the health facility | 109 | 100% | ||
| Organization | Only knows that the HMA has an ultrasound | 87 | 80% | 9.301 | 0.002 |
| Financing | Does not have a job | 39 | 36% | 4.649 | 0.031 |
| Organization | There was no availability of medications | 106 | 100% | ||
| Financing | Paid for medications privately | 90 | 85% | 59.27 | 0.000 |
| Financing | Paid for tests privately | 40 | 38% | 7.616 | 0.006 |
| Organization | Laboratory tests have been performed outside the hospital | 53 | 100% | ||
| Financing | Privately paid for exams | 23 | 43% | 6.641 | 0.01 |
| Organization | Has taken more than 60 minutes to be seen at the HMA oncology office | 91 | 100% | ||
| Financing | Does not have a job | 35 | 38% | 6.536 | 0.011 |
| Organization | Only knows that the HMA has an ultrasound | 72 | 79% | 5.289 | 0.021 |
| Perception | Has required more than one treatment in combination (Surgery, Chemotherapy or Radiotherapy) | 22 | 100% | ||
| Financing | Working | 21 | 95% | 8.597 | 0.003 |
| Demographic | Multifamily | 12 | 55% | 4.128 | 0.042 |
| Perception | Has moderate or severe anemia | 51 | 100% | ||
| Demographic | Schooling: Primary or None | 26 | 51% | 9.641 | 0.002 |
| Financing | to loans, sale of goods or two or more activities to finance their treatment | 23 | 45% | 6.742 | 0.009 |
DISCUSSION
The following study sought to determine the gaps in access to cancer treatment in the HMA in 2019 according to predisposing, enabling, and necessary factors.
According to the predisposing factors: regarding the most frequent type of cancer in the studied population, breast cancer was found in women with 49%, and digestive tract cancer in men with 37%, as the most prevalent. These tumors are among the four most frequent types in Lima (Peru) (17). These general findings could be related to the westernization habits of our population where there is little consumption of fruits and vegetables and little exercise; the influence of social determinants related to the poor quality of environmental sanitation services such as safe water, poverty, the consequently diminished possibility of improvements in living conditions and education, as we know, in these conditions there is a huge population in Peru, mainly in the medium-low economic stratum (18). The population that attends our institution frequently belongs to socioeconomic group E, where monthly economic income is an average of 1,300 Nuevos soles, even though the hospital is a reference hospital for the entire population of southern Lima, regardless of socioeconomic status (19). It should be noted that all the patients who were randomly selected had SIS and no other type of insurance.
When we evaluate predisposing factors such as age, those who are over 65 years of age suffer some type of access gap, these patients mostly require going to establishments accompanied by a family member, due to the high degree of dependency and if we relate it to cancer; it occurs more frequently in older adults, finding 21% of respondents in that age in our study, being considered and compared to the global estimate where more than 2 million cancers were diagnosed in adults 80 years of age or older in 2018, with breast, lung, colon and stomach cancers being the most common types in women, and prostate, lung, and colon cancer, the main ones among men worldwide, according to what was studied by Pilleron (20). Due to population aging, the estimated number of new cancer diagnoses is expected to triple by 2050 worldwide. A simple observation highlights the inextricable link between aging and cancer: the incidence curves for most common cancers are strikingly similar, rising after age 50, despite wide variation in the number of driver mutations. in these neoplasms and the fact that they originate from different groups of stem cells with great differences in size and organization. The current model of multistage carcinogenesis postulates that the exponential increase in cancer incidence with age results from the sequential accumulation of oncogenic mutations in a single clone. The Cancer Research UK website states that “advanced age is the main risk factor for cancer. This largely reflects cellular DNA damage that accumulates over time. (21–23)
Regarding gender, 74% of the study population corresponded to the female group, it is an expected finding given that women are the ones who use health services more frequently(10) we must also relate it to the prevalence of the type of cancer they suffer from, such as cervical and breast cancer (17) .
Regarding schooling, those who have primary or no education (table N ° 2.3), present limitations whose relationship is significant, when it is related to being over 65 years old (p: 0.000), and not having a job (p:0.001); We must understand that the economically active population is between 20 and 65 years old, and when they are diagnosed with cancer, this population is affected because the vast majority have to take time off work to receive treatment, and then they become more vulnerable due to the possibility of losing their jobs, coupled with the fact that more than 70% of the population belongs to the informal work group. (24–26) If we add to this that chemotherapies or oncological treatments somehow produce moderate or severe anemia (P:0.002) with a decrease in physical strength and that can negatively influence the person and their perception of work, which is why she is identified as not having a defined occupation (p:0.041). The finding of primary education or none behaves as an access gap, because people with this condition have less opportunity to understand about indications of care procedures or claim about their condition for timely care, contrary to those with education superior, who make their right prevail in terms of the opportunity to start treatment, the type of treatment to receive, this is corroborated by Riley (27) in his study on disparities in health care, where when relating it to age, we found that advanced age, older than 65 years, and low socioeconomic status or low income have a negative influence on health, increasing access gaps, in this case, access to cancer care (15).
Women have other limitations whose relationship is statistically significant, these are: Measuring less than 1.5 meters (p=0.020), not having a job (p= 0.042) and being afraid of surgical interventions (p=0.043). Short stature can be a limitation when structuring the types of treatment where the indications are carried out using the body surface, which is generally based on therapeutic schemes that have been designed in research studies or a basal protocol, carried out in a prototype of an individual, results that are extrapolated to our population, which may constitute a limitation or gap in our patients (28).
People who are afraid of a cancer diagnosis have limitations whose relationship is significant, these are: being afraid of surgical interventions (p=0.000), having feelings of helplessness to cancer (p=0.000), feeling ashamed to show their body at the time of the medical examination (p=0.011), and have needed to pay for examinations in a private way (p=0.038). There are fears and myths according to each cultural context as gaps that make it difficult to access cancer care (29,30), in this sense, psychological treatments of mind and body integration to manage uncertainties and fears would facilitate overcoming during diagnosis, and treatment and survival. of the patient, also with timely and accurate information to define the multidisciplinary treatment. All these processes produce fear and stress in cancer patients (31,32), however, in our establishments they are not managed in this way, which is why it is suggested to incorporate psychologists, nutritionists, rehabilitators and professionals who help mitigate this aspect.
However, since Supreme Decree 009-2012 was promulgated, where access to cancer services is promoted, there is financing from the Intangible Solidarity Fund for Health (FISSAL) for the types of cancer prioritized due to their high incidence, such as leukemia, lymphoma, breast cancer. , cervix, lymphoma, colon cancer, stomach, and those that are not in the Intangible Solidarity Fund for Health (33) are covered by the Integrated Health System (SIS), thus covering all the financing of neoplasms, all this is to mitigate the financial burden, however, if the establishment does not have the adequate equipment, the patient continues with the cost self-financed by them. Another problem is that it has not been possible to expand services at the level of public health establishments in three important areas such as specialized personnel, equipment, and infrastructure, which means that we have services with little resolution capacity, even though health establishments in general Both those of first level care and those of type II, III and specialized have not expanded in these components so that SIS affiliates struggle to find services in general and oncology services in particular; causing saturation of the service, delays in early diagnoses (screening strategies, imaging or histopathological detection tests) and initiation of treatment, with the high risk of affecting the timeliness and quality of patient care, even though the majority of the population is affiliated with comprehensive insurance (34,35) seeking universal health coverage. To comply with the provisions of the World Health Organization (WHO) on universal coverage, access to quality health services must be provided. For this, they must have an available supply of infrastructure, equipment, qualified personnel, and financial risk protection, and this is hardly it could be achieved in hospitals such as HMA because of the lack of basic equipment such as tomography and physical infrastructure due to the necessary physical spaces, mainly, lack of radiotherapy equipment, a fundamental pillar in cancer treatment, for which it is suggested to improve this type of shortcoming (34).
People who come from multi-family homes present a limitation whose statistically significant relationship, with: having required more than one treatment in combination to treat cancer (p=0.042), this would have as an explanation that patients who go to a public institution are generally of medium-low economic status where families are numerous, where they go to hospitals whose necessary resources such as imaging equipment such as tomography, resonance, necessary for the staging of malignant diseases are not available. (3)
According to the enabling factors: people who do not have a job present the following limitations such as: being over 65 years old (p=0.000), having studied primary school at most (p=0.001), having taken more than 60 minutes to be seen at HMA's Oncology office (p=0.011), having waited more than 24 weeks from the onset of their symptoms to receive care (p=0.031), all these indicators have to do with the level of education where they have basic education such as primary education limits the moment of getting a job, of being able to internalize the importance of seeking a health service to be screened for types of cancer that can be screened or when there are any symptoms; Likewise, these people may have limited knowledge or be unaware of their rights as a person and how to make them respect them in an indolent state that barely has the conditions to provide health care in an equitable manner, as mentioned in the following studies (36–38). In the situational analysis of cancer in Peru 2018 (3), we can see that many of these indicators found in the present study as a population with predominantly basic education such as primary, poverty that although it has a tendency to be decreased in the years 2007 to 2017 from 42.4 to 21.7% of the Peruvian population, have negative effects on chronic diseases, including cancer, since there is evidence that patients living in poverty are diagnosed with stage cancer advanced and are more exposed to risk factors. Therefore, it is important to prepare intervention strategies addressing social determinants to reduce disparities in health and prioritize communication strategies to mitigate these determinants. (39)
The people who have had to pay for tests in a private way present other limitations, these were: not finding availability of medicines (p:0.006), having carried out laboratory tests outside the hospital (p=0.010), having had to pay for medicines in an In particular (p=0.035), these conditions indicate that cancer patients are affected according to socioeconomic status, because the health system does not have the availability of infrastructure and equipment resources that allow them to provide quality and timely care . Among cancer patients and the general population, being afraid of a cancer diagnosis (p=0.038), and presenting difficulties in obtaining an appointment at the HMA Oncology office (p=0.039), behave as a barrier to obtaining the attention (10). Being afraid is a myth that makes it difficult for these people to go to health facilities and if this is added to the difficulty in finding an appointment, it causes cancer patients to miss out on treatment opportunities, and we know that in cancer it is crucial to provide timely treatment. (29,30) There are improvements in the financing of cancer patients through FISSAL and SIS; however, there has been no improvement in the implementation of more and better oncology services since universal health coverage has been implemented, so these patients continue to be impoverished with the expenses incurred and do not have the opportunity for treatment due to the lack of infrastructure and equipment (3,40).
People who have had to stop working as a result of a cancer diagnosis have limitations whose relationship is statistically significant, with: Having required more than one treatment in combination (surgery, chemotherapy or radiotherapy) (p=0.003), arguing that the treatments oncology are multidisciplinary in order to achieve the therapeutic objectives against the disease, so these patients probably have difficulties in continuing to work, recognizing that more than 70% of our economically active population has informal jobs, which limits them from having work break with the right payment. (26,36,37) They also have difficulties in getting an appointment at the HMA Oncology office (p=0.039), one of the probable causes may be the limited availability of specialists, being a problem that makes the diagnostic and treatment gaps are limited, which are enhanced because medical professionals and l Administrative staff do not have the training of specialists in the different oncological subspecialties, the training of these specialists is not prioritized, despite the fact that in the country the mortality rate is very high according to ASIS of cancer, for the years 2016 it is the second cause of death in Peru with 122 X 100,000 inhabitants (3).
People who have had difficulty getting an appointment at the HMA Oncology office have other limitations: not receiving the results of their laboratory tests on time (p=0.023), having stopped working (p=0.039) and being forced to pay their exams in a private way (p=0.039), as we see these interactions of organizational factors in the institution behave negatively in the required treatment, causing delays in appointments, going to the establishment more times generating inconveniences in their work, in having to have a companion.(7,15) PTherefore, it is suggested that the health establishment should improve the organization of its processes, in such a way that a patient-centered service can be provided. To this we must add that there are people who have waited more than 24 weeks (the maximum waiting time observed in the sample) from the onset of their symptoms to going to a health facility (p=0.002), which shows us how little adherence to the preventive culture of our population and diagnosis in advanced stages, where therapeutic interventions have little effectiveness and the possibility of cure is minimal.
According to the necessary factors, anemia, especially of moderate-severe severity, behaves as a gap in access in cancer patients, since it behaves as a disability because it makes it impossible for the patient to fend for himself, this is reported by Owusu, (41) where they found that a cohort of people older than 65 years with anemia was independently associated with functional disability and that the independent association between anemia and functional disability was not explained by sex, cancer stage or unintentional weight loss in the last six months. Older patients with cancer and anemia (compared to those without anemia) were more than twice as likely to have functional disability due to presenting multifactorial anemia. (16,41)
People who had the need to require more than one treatment in combination (surgery, chemotherapy or radiotherapy) present other limitations whose relationship is statistically significant, these are: Stop working (p=0.003) and come from a multi-family household ( p=0.042). When the patient stops working, it limits her economic condition, and if she comes from a multi-family home, this condition worsens since she will have to distribute the economic precariousness among various components of the family. (24,26,37)
Within the limitations of the study, we have that it was a study based on the perception of patients to measure access gaps, neither the specific staging nor the survival of the patients was taken into account. For this reason, prospective analytical studies are suggested that can measure other variables such as type of cancer, staging, associated factors, survival and thereby contrast their relationship with the access gaps already analyzed in this first work. This work was the beginning of future work in the hospital, specifically according to the type of neoplasia in our context.
CONCLUSIONS
There is a significant gap for cancer care such as those concerning predisposing factors (fear of diagnosis, feelings of helplessness, being female, being over 65 years of age (p=0.000), and having primary education or not having studies) ; enabling factors (unavailability of medications, paid for tests in a private way, waiting more than 24 weeks from the onset of symptoms to going to the health facility, difficulty getting an oncology appointment, spending between 501 and 1,000 soles, not having a job, non-timely delivery of laboratory test results, not having a job, paid for tests in a private way, stop working, payment for drugs in a private way, two or more activities to finance their treatment) and for the necessary factors (having moderate to severe anemia or have required more than one treatment in combination).
Autorship contributions: Reina Bustamante-Coronado, José M. Vela-Ruiz, Ricardo A. Carreño-Escobedo have participated in the conception of the article, data collection, writing, and approval of the final version. In addition, Omar Paredes-Olivares performed the data analysis.
Funding Source: Self.
Conflict of interest: The authors declare no conflict of interest.
Received: February 06, 2022
Approved: June 15, 2022
Correspondence Reina Bustamante-Coronado.
Address: Av. Miguel Iglesias 968 , Hospital María Auxiliadora – Dpto Oncología (5to piso).
Telephone: +51 999916543
E-mail: r.bustamante312@gmail.com
Artículo publicado por la Revista de la Facultad de Medicina Humana de la Universidad Ricardo Palma. Es un articulo de acceso abierto, distribuido bajo los términos de la Licencia Creatvie Commons: Creative Commons Attribution 4.0 International, CC BY 4.0(https://creativecommons.org/licenses/by/1.0/), que permite el uso no comercial, distribucion y reproducción en cualquier medio, siempre que la obra original sea debidamente citada. Para uso comercial, por favor póngase en contacto con revista.medicina@urp.edu.pe.
REFERENCIAS
