CARTA AL EDITOR
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2022 - Universidad Ricardo Palma10.25176/RFMH.v22i2.4805
ADDITIONAL COMMENTS TO THE ARTICLE WRITTEN BY EYMARD TORRES-RODRIGUEZ ET AL: REDUCTION OF CARDIOVASCULAR RISK IN OBESE PATIENTS WHO PARTICIPATED IN A LIFESTYLE MEDICINE PROGRAM
COMENTARIOS ADICIONALES AL ARTÍCULO DE EYMARD TORRES-RODRIGUEZ ET AL: DISMINUCIÓN DEL RIESGO CARDIOVASCULAR EN PACIENTES OBESOS QUE PARTICIPARON EN UN PROGRAMA DE MEDICINA DE ESTILO DE VIDA
John C. Longa López1,a
1 Instituto de Investigación en Ciencias Biomédicas (INCIB), Universidad Ricardo Palma, Lima-Perú
a Especialista en Endocrinología. Maestría en Salud Pública con mención en Gestión Hospitalaria
Chronic diseases have occupied a leading place in global morbidity and mortality statistics, given the increase in life expectancy and access to new therapeutic technologies and advanced drugs. Cardio-metabolic diseases such as diabetes, high blood pressure, dyslipidemia, and obesity, among others, are clear examples of both the impact and the advent of new therapeutic opportunities. In this study, the effect of a lifestyle program on the cardiovascular risk of enrolled patients was evaluated.
In the present study, it is noteworthy that patients with stage 3 and 2 arterial hypertension, for example, apparently passed to lower stages. Still, it is not mentioned whether they received pharmacological treatment, which was mandatory in this degree of arterial hypertension, given its magnitude. : if he did not receive it, it was a regrettable omission, and if he did receive it, then the pharmacological control was not adequate, and we cannot attribute the drop in blood pressure only to the lifestyle program. Another aspect that draws a lot of attention is the decrease in the reported body mass index, in which there is a decrease in the percentage of fat but especially in muscle mass, which constitutes an "unwanted" outcome that could lead to what we call sarcopenic obesity, with the dire consequences in cardiovascular risk that have the loss of muscle mass. An important limitation is the fact that patients are not given basal glucose, a variable with a high impact on cardiovascular risk since, being obese, it was necessary to rule out diabetes in this group to better stratify it.
The present author has allowed himself to do an exercise to assess long-term cardiovascular risk with the changes achieved by the program cited in this study to see the impact of this intervention on cardiovascular mortality over more than 10 years, using the QRISK Lifetime Cardiovascular Risk Calculator and using the mean values of the entire group (n=9) obtained after 6 months of intervention reported in the tables presented. Thus, a patient with an average age of 51 years (reported in the study), a non-smoker (since none of the group was a smoker), with a total/HDL cholesterol ratio of 5.27 and 4.98, before and after the intervention (the average LDL-C reported by the study and an average valuemg/dlof 40 of HDL-C before and after the intervention have been considered, the latter parameter that was not evaluated in the present study and that constitutes a limiting) with a systolic pressure of 132 and 124 mmHg (before and after the intervention, respectively, values reported by the study) and a weight of 109 and 106 kg (before and after the intervention reported by the study) have the following curves projection of cardiovascular risk: 44.3 41.2.
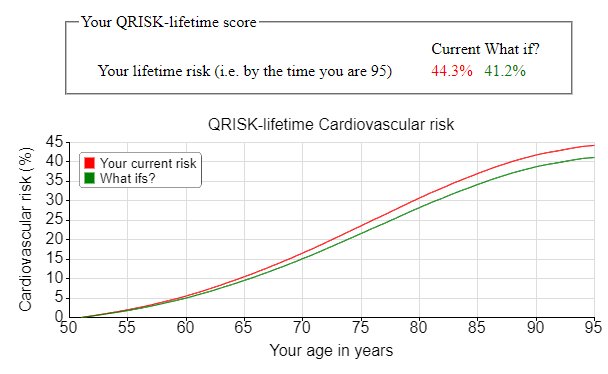
Note that the cardiovascular risk curves only begin to separate above 60 years of age, which tells us about the need for long-term sustainability of interventions to really have a signicant impact.
Finally, there is no doubt that changes in lifestyle are a fundamental pillar for the prevention of many chronic diseases and that cardiovascular risk stratication allows the proling of each patient towards the practice of individualized medicine with a preventive approach.
Authorship contributions: The author analyzed andthe preparation of the manuscript of
this article.
Conflicts of interest: Self financed.
Conflictos de interés: The author declares not havingconict of interests.
Received: February 16, 2022
Approved: March 03, 2022
Correspondence: John Carlos M. Longa López
Address: Calle Doña Nelly 566 dpto 401- Urb. Santa Rosa de Surco, Surco,
Lima-Perú.
Telephone number: 959912710
E-mail: johnlonga@gmail.com
REFERENCES
