REVIEW ARTICLE
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2023 - Universidad Ricardo Palma10.25176/RFMH.v23i4.5877
MORTALITY OF PATIENTS HOSPITALIZED BY COVID-19 IN MEXICO, SYSTEMATIC REVIEW
MORTALIDAD DE PACIENTES HOSPITALIZADOS POR COVID-19 EN MÉXICO, REVISIÓN SISTEMÁTICA
Ana Portocarrero Granados
 a
a
Lya Angélica Castro Rodríguez
a
Antonio Sandoval Cabrera
b
María del Socorro Romero Figueroa
a,c
a Facultad de Medicina, Coordinación de Investigación, Campus Universitario Siglo XXI, Zinacantepec México
b Investigador, Hospital para el niño del Instituto Materno Infantil del Estado de México
c Investigador Asociado de la Universidad Anáhuac México, Centro de Investigación en Ciencias de la Salud Lomas Anáhuac 786, Huixquilucan, México
ABSTRACT
Introduction: Since the start of the pandemic, Mexico was one of the countries with the highest mortality rates from COVID 19.
Objective: To determine if type 2 diabetes mellitus, arterial hypertension, and obesity increase mortality in patients diagnosed with COVID-19 who required hospitalization in Mexico.
Methods: Systematic review in Pubmed MeSH, Web of Science, Lilas, Scielo, and Google Scholar with the terms MeSH COVID-19, SARS-COV2, Coronavirus, and Mexico for the years 2020 and 2021, in English or Spanish. Two reviewers selected the studies, two additional reviewers participated in the analysis of the studies.
Results: Seventy three studies carried out in Mexico from 2020 to 2021 were included with information obtained from the databases of the National Epidemiological Surveillance System of Mexico. With an average age of 52.9 ± 13.27 years, 64% of the included patients were women, in general, a mortality rate of 16.76% (Min-Max 0.77-73.73%) was reported. 71% of the studies (52) did not report specific mortality related to comorbidities the most prevalent pathology was obesity with 24.23% (Min-Max 11.50-71.00%), followed by arterial hypertension 22.23% (Min-Max 2.0-53.96%) and finally Diabetes mellitus with 18.10% (Min-Max 1.83-40.00%).
Conclusion: The most common comorbidity among patients hospitalized for COVID in Mexico was obesity, followed by type 2 diabetes mellitus and hypertension.
Keywords: COVID 19, diabetes, hypertension, Mexico, mortality, obesity. (Source: MESH-NLM)
RESUMEN
Introducción:
Desde el inicio de la pandemia, México fue de los países que presentó tasas de mortalidad más altas por COVID 19.
Objetivo:
Determinar si la diabetes mellitus tipo 2, la hipertensión arterial y la obesidad incrementan la tasa de mortalidad en pacientes con diagnóstico de COVID-19 que requirieron hospitalización en México.
Métodos:
Revisión sistemática en Pubmed MeSH, Web of Science, Lilas, Scielo y Google Scholar con los términos MeSH “COVID-19”, “SARS-COV2”, “Coronavirus”, y “México” durante los años 2020 y 2021, incluyendo artículos en inglés y español. Para el proceso de selección de artículos, dos revisores seleccionaron los estudios mientras que otros dos revisores adicionales participaron en el análisis de dichos estudios.
Resultados:
Se incluyeron 73 estudios realizados en México del 2020 al 2021 con información obtenida a través de las bases de datos del Sistema Nacional de Vigilancia Epidemiológica de México. Se incluyeron pacientes con un promedio de edad de 52,9 años ±13,27, el 64% de los pacientes incluidos fueron mujeres, se reportó una tasa de mortalidad de 6.76% (Min-Max 0.77-73.73%). El 71% de los estudios (52), no reportaron la mortalidad específica relacionada con las comorbilidades. La patología más prevalente fue la obesidad con un 24.23% (Min-Max 11.50-71.00%), seguida de la hipertensión arterial con un 22.23% (Min-Max 2.0-53.96%) y finalmente la diabetes mellitus tipo 2 con un 18.10% (Min-Max 1.83-40.00%).
Conclusión: La comorbilidad más común entre los pacientes hospitalizados por COVID 19 en México fue la obesidad, seguida de la diabetes mellitus tipo 2 y por último la hipertensión.
Palabras clave: COVID 19, diabetes, hipertensión, México, mortalidad, obesidad. (Fuente: DeCS- BIREME)
INTRODUCCIÓN
Since the WHO declared a pandemic on March 11, 2020, until December 30, 2022, a total of 7,639,825 COVID-19 cases and 345,639 deaths were confirmed, ranking fifth (1) in the world in terms of reported deaths.
Throughout the pandemic, sufficient evidence emerged suggesting that the severity of clinical manifestations and the disease's mortality rate vary from person to person, depending on factors such as advanced age (people over 70 years), obesity, the presence of comorbidities like diabetes mellitus, hypertension, renal disease, and diseases associated with immunosuppression and systemic inflammation (2-4).
Given that in Mexico, 36.1% of adults over 20 years of age are obese (5) and approximately 10.32% (8,542,718) have diabetes mellitus (6), during the entire pandemic Mexico remained one of the top five countries with the highest mortality rate worldwide. Hypertension, obesity, and type 2 diabetes mellitus increase the vulnerability to develop severe complications due to SARS-CoV-2 infection and are discussed below.
Systemic Arterial Hypertension
ACE2 (angiotensin-converting enzyme 2) has been recognized as the binding receptor for SARS-CoV-2 at the onset of the infectious process in a host cell. This binding is achieved through the recognition of the RBD domain belonging to the S1 subunit of the viral S protein. The distribution and presence of ACE2 in human body tissues could act as potential viral targets and, therefore, be susceptible to infection. This receptor has been highly identied in type II alveolar epithelial cells of the lung, brain, and enterocytes of the small intestine (7).
ACE2 (angiotensin-converting enzyme 2) is a secreted and membrane-associated aminopeptidase expressed in various tissues (8). Discovered in 2000 as a homolog of the angiotensin-converting enzyme (ACE) (9), it has a potent negative regulatory action on the reninangiotensin system (RAS), which plays a signicant role in cardiovascular physiology and homeostasis through the regulation of electrolyte balance, blood pressure and vascular tone (10,11). Dysfunction of the RAS results in elevated levels of angiotensin II, a vasoactive peptide with vasoconstrictive and inflammatory properties, increasing the number of macrophages and their infiltration into the vascular wall, thereby raising immune cell numbers and inammation, contributing to increased oxidative stress (10).
In various animal models and human studies, it has been demonstrated that chronic administration of renin-angiotensin system (RAS) inhibitors increases the expression of ACE2. This suggests the possibility of higher susceptibility to SARS-CoV-2 infection and a more severe disease course with the use of RAS inhibitors (12).
The endothelium, lining the inner wall of vessels and being the primary regulator of vascular homeostasis, modulates the balance between vasoconstriction/vasodilation, inhibits the proliferation/migration of vascular wall muscle cells, and also modulates hemostasis. Endothelial dysfunction is an event that precedes the morphological changes characteristic of atherogenesis and contributes to the development of complications of atherosclerotic plaque (13).
This common denominator is most prevalent among COVID-19 comorbidities. In hypertension, sustaine delevation of systemic pressure in the microvasculature leads to premature aging and increased turnover of endothelial cells, affecting the endothelium's ability to release endothelium-derived relaxing factors, causing vasoconstriction (14). Endothelial dysfunction is suggested to be involved in COVID-19 progression due to atypical manifestations among patients, such as cardiac injury and hypercoagulability, indicated by increased levels of D-dimer and Von Willebrand factor. Common inammator y markers obser ved in endothelial dysfunction, including C-reactive protein, IL-6, and TNF-alpha, are also elevated in COVID-19 patients (15). The mechanical stress caused by high intraluminal pressure in the vascular wall activates NADPH oxidase (NOX), the main enzyme producing reactive oxygen species, triggering oxidative stress leading to endothelial dysfunction. This oxidative stress incites a destructive cascade in the arterial wall followed by chronic inammation resulting in changes in the arterial wall, such as remodeling, increased intimamedia thickness, and functional remodeling (16).
Obesity
Overweight and obesity are major health issues in Mexico (17). According to the latest "National Health and Nutrition Survey 2020," the combined prevalence of overweight-obesity in adults over 20 years was 76.8% in women and 73.0% in men (18).
Obesity, along with other diseases like diabetes mellitus or hypertension, are risk factors and increase mortality due to COVID-19. These conditions are associated with hypertrophy and hyperplasia of adipocytes, which disrupt the balance in the production of adipokines, inducing the secretion of pro-inammatory adipokines such as leptin, interleukins (IL-1β, IL-6, and IL-8), TNF-α, MCP-1, and decreasing the production of anti-inammatory adipokines like adiponectin (18,19). These cytokines cause low-grade inammation and a dysfunction of innate immunity, predisposing to the development of infections.
Leptin acts on pulmonary broblasts and contributes to lung inammation by inducing pro-inammatory cytokines and chemokines, with high leptin levels associated with more severe lung inammation in COVID-19 patients. There is a positive correlation between the duration of SARS-CoV-2 infection and the degree of interstitial brosis; pulmonary brosis due to an excess of extracellular matrix components produced by activated myobroblasts poses a barrier to gas exchange (20).
The cellular receptor for SARS-CoV-2, besides being expressed in the heart, vessels, lungs, kidneys, testicles, and brain, is also present in adipose and lung tissues in obese patients (21).
Elevated expression of angiotensinconverting enzyme by adipose tissue promotes greater viral replication, and adipose tissue can act as a reservoir and storage for the virus. These patients are more susceptible to thromboembolic episodes due to hypercoagulability (22).
Obesity also leads to a procoagulant state, which can be exacerbated by SARSCoV-2 infection, thus leading to worse clinical outcomes (23).
The function of various immune cells is also altered in obese patients; obesity affects the responses of T and B cells, thus delaying the adaptive immune response to infection. The weakened immune system in obese patients can result in a higher viral load, rapid replication, and viral spread (24).
From a physiological perspective, obesity impairs respiratory mechanics and gas exchange, increases airway resistance, and reduces the strength of respiratory muscles and lung volumes (25).
Type 2 Diabetes Mellitus
Diabetes is the second underlying cause of death in Mexico, accounting for 14% of deaths (26,27). A metaanalysis including 33 studies reported a correlation between diabetes mellitus and disease severity, with more patients requiring invasive ventilation and ICU admission, leading to higher mortality in this group (28).
Poor glycemic control in patients with type 2 diabetes mellitus is associated with magnesium deciency and a subacute proinammatory state, including increased circulating proinammatory cytokines and altered levels of lymphocytes, neutrophils, and macrophages compared to non-diabetic subjects (29,30).
This lived experience underscores the need for prevention in the face of a future pandemic of this magnitude. Together, these observations indicate that to reduce the impact of SARS-CoV-2, a broad approach is required; interventions must address not only virus transmission but also a comprehensive assessment of a population's health status.
Therefore, the aim of this study was to determine if type 2 diabetes mellitus, hypertension, and obesity increase mortality in patients diagnosed with COVID-19 in Mexico
METHODS
Search Strategy
A systematic review was conducted in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analysis) guidelines of articles published from January 2020 to December 31, 2021 in English or Spanish.
The systematic search was performed in the following databases using Boolean operators: PubMed MeSH (Medical Subject Heading) ("COVID-19"[MeSH] or "Mexico"[MeSH]) or ("diabetes mellitus" [MeSH] or "obesity" [MeSH] or "Hypertension"[MeSH] or "Mortality"[MeSH]), Scopus (Mexico and COVID-19 or CORONAVIRUS or SARS-CoV-2 or SARS) or (diabetes, obesity, and hypertension or mortality or comorbidity), Web of Science Mexico (title) and COVID-19 (all elds) and (diabetes or hypertension or obesity or mortality (all elds) and comorbidities), Lilas (Mexico and (COVID-19 or SARS-CoV-2 or Coronavirus)), Google Scholar (Mexico and (COVID-19 or SARS-CoV-2 or Coronavirus)), and Scielo (Mexico and (COVID-19 or SARS-CoV-2 or Coronavirus)). The MeSH terms used were: "review" or "literature review" or "Meta-Analysis", type of publication].
Studies without an abstract or full text were excluded. When an abstract met the inclusion criteria, which included hospitalized patients over 20 years old, with reports of the three
comorbidities studied (obesity, hypertension, and
diabetes mellitus) as well as mortality, the full text was
reviewed. All selected articles were identied and
reviewed by four authors (AP, LC, AS, SR).
Data Collection and Analysis
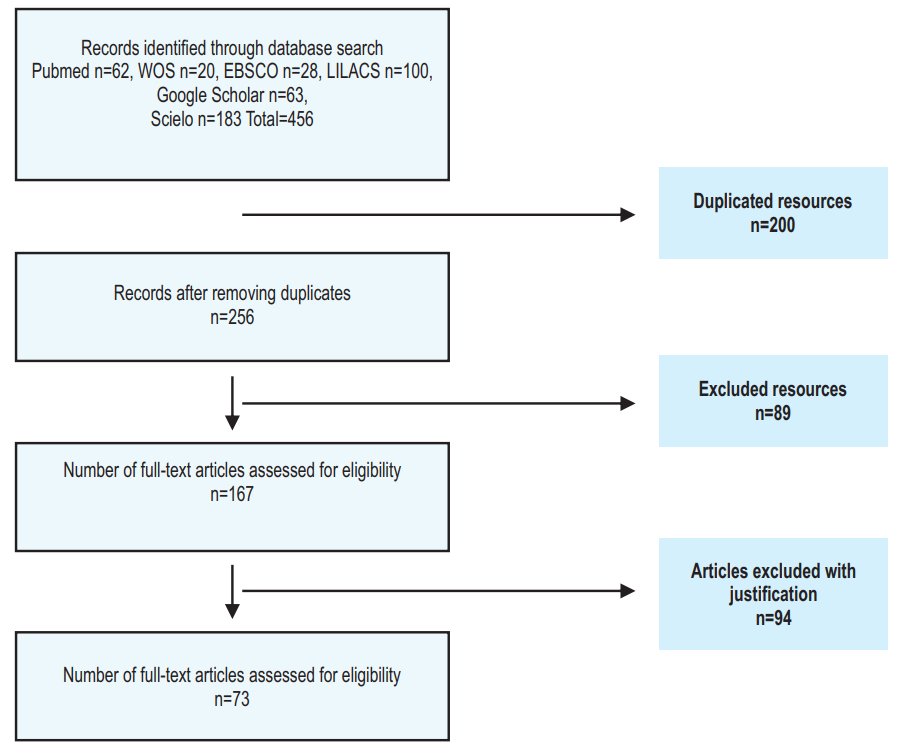
Data extraction and management were performed by two independent reviewers (AP, LC). To assess whether studies met the inclusion criteria, two additional reviewers were involved in analyzing the studies (AS, SR). The study selection process is presented in Figure 1. The information extracted and analyzed from the collected studies included the year of study, number of cases included, number of diabetic patients, number of hypertensive patients, number of obese patients, and number of deceased patients. Results are summarized narratively in each relevant section within the text of this review.
The results are summarized narratively in each relevant section within the text of this review.
RESULTS
After searching the databases, a total of 456 studies were found. 200 duplicate records were removed, and 89 articles were excluded for not meeting selection criteria upon full article review. In a second review, two independent reviewers excluded some articles for presenting incomplete results or being studies on the pediatric population. Finally, 73 studies were included for analysis.
Characteristics of the Included Studies
The 73 included studies were conducted in Mexico, between 2020 and 2021. Most obtained information from national databases like the National Epidemiological Surveillance System with 24 studies (32.8%), and local databases like those of the National Institute of Respiratory Diseases with 20 studies (27.3%), the Ministry of Health with 19 studies (26%), and the Mexican Institute of Social Security with 10 studies (13.6%). 64% of the study population were women, with a median age of 52.9 years SD ±13.27.
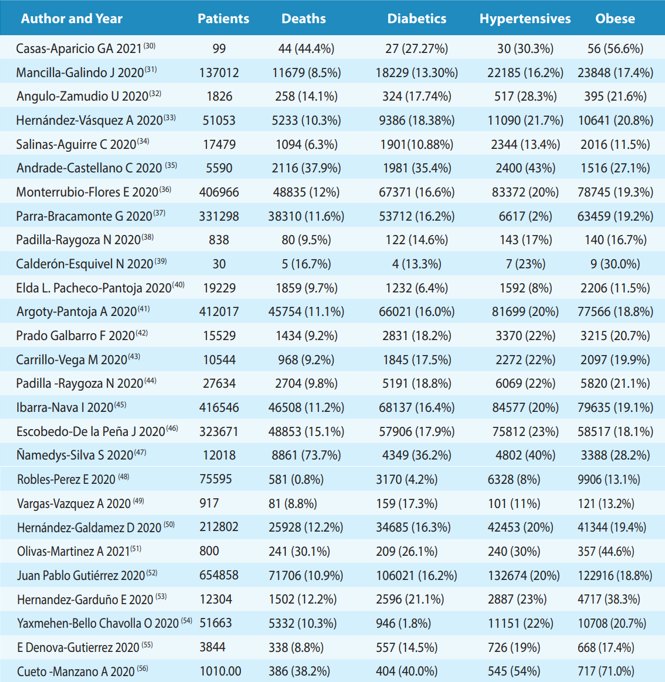
The characteristics of the studies are presented in Table 1. Generally, a mortality rate of 16.76% (Min-Max 0.77-73.73%) was reported. 71% of the studies (n=52) did not report specic mortality related to comorbidities. The most prevalent pathology was obesity with a rate of 24.23% (Min-Max 11.50-71.00%), followed by hypertension 22.23% (Min-Max 2.0-53.96%), and nally diabetes mellitus with 18.10% (Min-Max 1.83-40.00%).
DISCUSSION
The global spread of Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV-2) triggered an economic and health crisis worldwide.
Since the beginning of the pandemic, Mexico ranked among the top 5 countries in morbimortality, as severe COVID-19 disproportionately affects people over 70 and patients with comorbidities such as obesity, diabetes, hypertension, cardiovascular disease, chronic kidney disease, and chronic lung disease (1,5), prevalent in Mexico.
The pandemic highlighted a high prevalence of undiagnosed type 2 diabetes mellitus, showing a higher risk of mortality than previously diagnosed cases. Patients with overweight/obesity and COVID-19 required more ICU admissions due to a greater need for intubation, longer hospital stays, and exhibited higher mortality compared to individuals with a BMI between 18.5 and 25 kg/m². Hospital saturation and long care times also led to increased mortality (23,25).
Other factors inuencing these outcomes include Mexico's large population, with approximately 42% living in poverty (5), lacking easy access to health institutions.
50% of the Mexican population is not affiliated with Social Security, relying on state or federal health services or expensive private services (31). This health inequality due to poverty may be linked to a¿ higher risk of dying from COVID-19. Social vulnerability played a decisive role, as isolated communities lack adequate access to the health system(32).
Mexico had one of the lowest COVID-19 diagnostic test rates per capita in the world (about 17 tests per 1000 people)(33).
The pandemic management by health authorities faced criticism, with initial controversy over mask use and open international borders, which might have contributed to case numbers but not consistently to mortality.
The SARS-CoV-2 vaccination campaign in Mexico started in December 2020, targeting healthcare workers and older adults, with 63% of the population immunized by late 2021. This resulted in a reduction in severe and hospitalized COVID-19 cases, but an increase in mortality probability among hospitalized patients, mainly unvaccinated individuals (34).
CONCLUSIONS
Age, gender, and comorbidities such as diabetes, obesity, and hypertension were the most frequently associated risk factors for death from COVID-19.
Demographic differences, comorbidity prevalence, healthcare capacity, and effectiveness of risk mitigation measures impact mortality and complications from COVID-19.
The Mexican health system's efforts should focus on promoting healthy lifestyles to achieve better metabolic control in diabetic and hypertensive patients, as an association between glycemic dysregulation and the severity of respiratory disease caused by SARS-CoV-2 was documented.
Autorship contributions:
All authors participated in the conception, preparation and approval of the final version of the manuscript.
Funding:
Self-funded.
Conflict of interest:
The authors declare that they have no interest conflict.
Received:
August 18, 2023.
Approved:
December 5, 2023
Correspondence:
María del Socorro Romero Figueroa. PhD.
Address:
Universidad Anáhuac México, Centro de Investigación en Ciencias de la Salud Lomas Anáhuac 786, Huixquilucan, México, Ex Hacienda Barbabosa 36 A Zinacantepec, México. CP 51356.
Phone:
+52 7224745083
E-mail:
sromero61@hotmail.com
Article published by the Journal of the faculty of Human Medicine of the Ricardo Palma University. It is an open access article, distributed under the terms of the Creatvie Commons license: Creative Commons Attribution 4.0 International, CC BY 4.0 (https://creativecommons.org/licenses/by/1.0/), that allows non-commercial use, distribution and reproduction in any medium, provided that the original work is duly cited. For commercial use, please contact revista.medicina@urp.edu.pe.
BIBLIOGRAPHIC REFERENCES
