ORIGINAL ARTICLE
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2024 - Universidad Ricardo Palma
1 Hemotherapy and Blood Bank Service of the Hospital Nacional Cayetano Heredia.
2 Universidad Peruana Cayetano Heredia.
3 Universidad Científica del Sur.
4 Internal Medicine Unit, Mount Sinai Beth Israel Hospital.
5 Immunology Laboratories, Universidad Peruana Cayetano Heredia.
a Medical surgeon.
b Pharmaceutical chemist.
c Medical technologist.
d Student.
e Rheumatologist.
ABSTRACT
Introduction: Obesity and overweight constitute global public health challenges, negatively
impacting more than one billion people. They are accompanied by significant psychological and social
consequences, including the stigma associated with weight, with severe repercussions on mental and
physical well-being. Health professionals are directly involved with this problem; however, few studies
address weight stigma in Chile.
Objective: To examine the association between nutritional status (BMI) and the level of weight
stigma in university students of health careers in the region of Ñuble, Chile.
Methodology: Cross-sectional descriptive observational design. The GAMS-27 scale was applied to
assess weight stigma and BMI to evaluate the nutritional status of 156 students of health careers. Chi2
tests of independence and binary logistic regression were applied to evaluate the association between
the variables, with the R statistical package version 4.3.0.
Results: A statistically significant association was found between weight stigma and nutritional
status (p=0.0145). Presenting normal BMI (p=0.0163) and being female (p=0.0156) were associated with a
higher probability of presenting weight bias.
Conclusions: The present study identified a statistically significant association between weight
stigma and nutritional status in college students. It is vital to promote education regarding weight
stigma in college students to avoid bias and improve respect for future users.
Keywords: weight prejudice, nutritional status, students, health occupations. (Source: MeSH NLM).
RESUMEN
Introducción: El uso de sangre de cordón umbilical (CU) tiene muchas ventajas en la medicina
regenerativa. El plasma rico en plaquetas (PRP) es una fuente de factores de crecimiento en donde su
dinámica en el tiempo ha sido evaluada en sangre periférica, sin embargo, su evaluación en sangre de CU
no ha sido estudiada.
Objetivo: Evaluar la cinética de la liberación del PDGF-BB del PRP obtenido de sangre de CU.
Materiales y métodos: Se realizó un estudio experimental in vitro. Se recolectaron muestras de
sangre de CU de 6 partos a término de gestantes sanas que tenían entre 18 y 36 años y que acudieron al
Hospital Cayetano Heredia en Lima-Perú. Las muestras obtenidas se centrifugaron a 900 g durante 10
minutos para preparar el PRP. La activación se realizó con gluconato de calcio (GLu.Ca) al 10% y se
dividió en 4 alícuotas: (i) sin activador; (ii) 1 hora; (iii) 24 horas; (iv) 48 horas. La cuantificación
del PDGF-BB fue evaluada mediante el método de ELISA.
Resultados: La media (desviación estándar) de la concentración de PDGF-BB medida a la hora, 24
horas y 48 horas fue 6127.9 ± 101.6 pg/mL, 6197.5 ± 34 pg/mL y 6176.8 ± 63.3 pg/mL, respectivamente. La
cinética del PDGF-BB liberado por el PRP mostró valores constantes durante las 48 horas.
Conclusiones: La liberación de PDGF-BB del PRP obtenido de sangre de CU se indujo rápidamente y
se mantuvo constante y de forma mantenida durante las primeras 48 horas luego de su activación.
Palabras clave: Plasma rico en plaquetas; factor de crecimiento derivado de plaquetas; cinética;
sangre de cordón umbilical.
Platelets are blood components that play an important role in cell regeneration through the release of growth factors (GF), cytokines, and inflammatory response (1,2). The main GFs released by the alpha granules of platelets are platelet-derived growth factor (PDGF) and transforming growth factor-β (TGF-β), which are responsible for cellular chemotaxis, angiogenesis, and extracellular matrix production (3,4). Epidermal growth factor (EGF, fibroblast proliferation) and vascular endothelial growth factor (VEGF, angiogenesis) are other factors released by platelets that together play an important role in hemostasis, proliferation, and remodeling during the different phases of wound healing (5).
Platelet-rich plasma (PRP) therapy has gained popularity in regenerative medicine due to its potential to provide a high concentration of GFs (6). PRP is an autologous blood component that contains a high number of platelets and is typically obtained from peripheral blood (7). It is used in various clinical fields such as traumatology, ophthalmology, dentistry, cosmetic surgery, and wound healing, serving as a therapy to enhance tissue regeneration (8). However, its use has some drawbacks, such as the method of obtaining it, which can cause pain or injury to nerves or blood vessels at the puncture site (9,10). Additionally, in patients with compromised immune systems, there may be an abnormal expression of growth factors, potentially impairing their regenerative function (11).
PRP can also be easily obtained from umbilical cord (UC) blood. The comparison between peripheral blood and UC blood will differ in both the type and quantity of growth factors they contain (12). Studies mention that PRP obtained from UC blood has therapeutic advantages over that obtained from peripheral blood as it contains a higher concentration of GFs. Buzzi et al. (13) compared the GF content of UC and peripheral blood, finding higher levels of EGF, TGF-β, PDGF, and VEGF in UC samples. This is similarly demonstrated by Murphy et al. (3) and Parazzi et al. (14). The former showed higher values of PDGF-BB and VEGF (p<0.01) in PRP from UC blood, while the latter reported elevated concentrations of angiogenic factors (VEGF, growth hormone, erythropoietin, and resistin) in platelet gel prepared from UC blood compared to peripheral blood.
The concentration of GFs released from PRP varies over time, with kinetics studies determining the speed at which they reach their maximum concentration (15). Roh et al. (2), using PRP from peripheral blood, observed that the levels of factors such as PDGF-BB and VEGF remained constant for 7 days, suggesting that these findings would be useful in guiding PRP treatment in regenerative medicine. Despite the widespread use of PRP with GFs to enhance wound healing and tissue regeneration, little is known about its kinetics when obtained from UC blood. This study could provide insights into its behavior and potential therapeutic utility. Therefore, the objective of this study is to evaluate the release of PDGF-BB from PRP obtained from UC blood at different time points.
METHODSAn in vitro experimental study was conducted to evaluate the kinetics of PDGF-BB release in PRP obtained from UC blood from term deliveries attended at the Obstetrics and Gynecology Service of the Hospital Nacional Cayetano Heredia during May 2023.
Population and sampleUC blood samples were collected from 6 term deliveries of healthy pregnant women aged between 18 and 36 years who had previously agreed to participate and signed an informed consent form. Pregnant women with a history of blood disorders, metabolic disorders (diabetes mellitus, obesity, etc.), hemoglobin < 11 g/dL, platelets < 150 x 10^3 µL, autoimmune diseases, concomitant medication such as antiplatelet agents, corticosteroids, or nonsteroidal anti-inflammatory drugs in the last 15 days, or inflammatory or infectious processes according to medical history were excluded from the study.
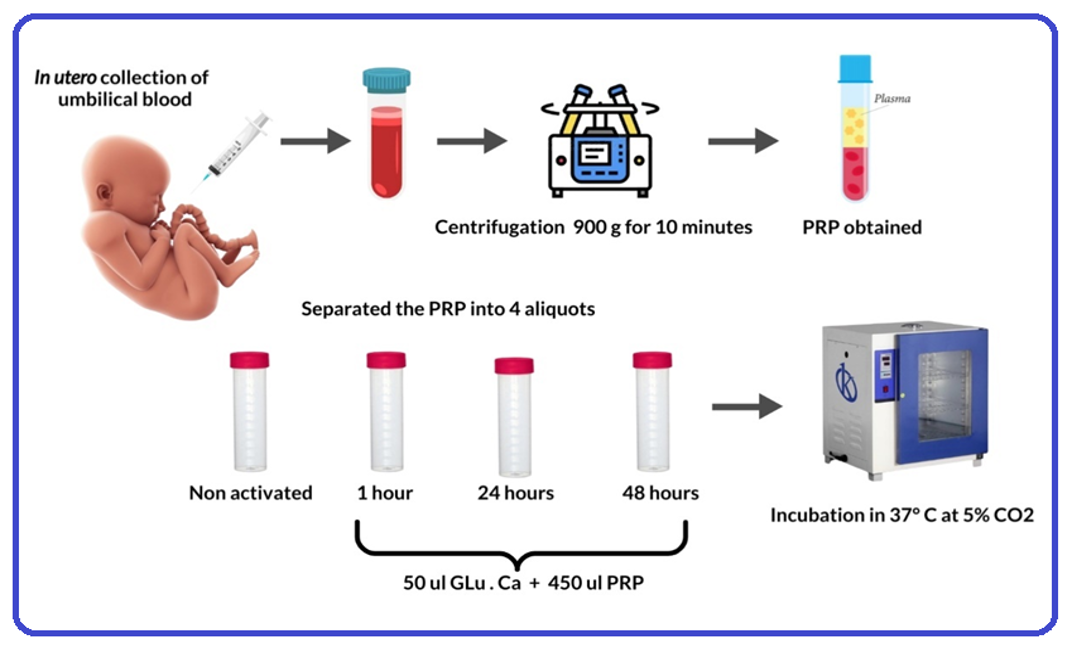
ProceduresIn utero collection was performed, where, once the newborn was delivered and assessed, the cord was clamped and cut, and blood was collected. A total of 7 cc of UC blood was collected into tubes containing 3.2% sodium citrate anticoagulant after puncturing the umbilical vein with a syringe. This procedure took less than 5 minutes. The samples were then taken to the Hemotherapy and Blood Bank Service for processing, where basal platelet counts were performed before centrifugation using the CELL-DYN Emerald hematology analyzer from Abbott.
Preparation and activation of PRPThe collected samples were centrifuged at 900 g for 10 minutes. After centrifugation, the lower third of the obtained plasma, corresponding to PRP, was separated and transferred to a sterile glass tube to perform post-centrifugation platelet counts. The PRP was then activated with 10% calcium gluconate (Glu.Ca) at 10%. The PRP was divided into 4 aliquots and labeled as follows: (i) without activator, (ii) 1 hour, (iii) 24 hours, and (iv) 48 hours. In a proportion of 1/10, 50 µL of Glu.Ca and 450 µL of PRP were added to aliquots (ii), (iii), and (iv). Each group, except for (i), was incubated at 37°C and 5% CO2 for 1 hour, 24 hours, and 48 hours, respectively. After the incubation period, they were stored in a -40°C freezer for subsequent measurement of PDGF-BB (Figure 1).
Figure 1: Workflow for the collection, processing, and distribution of PRP from umbilical
cord blood.
Source: Own elaboration.
The determination of PDGF-BB was performed using the Human PDGF-BB ELISA Kit (Product Number: RAB0397; Lot Number: 1128JO180) from Sigma Aldrich, which utilizes the Sandwich ELISA methodology.
The preparation of the standard was done according to the insert's specifications. The standard curve was obtained by serial dilution. The dilutions of the standard curve were performed in duplicate, and the average values for each dilution were obtained, after subtracting the blank as a control, to construct the standard curve from the values read on a BioTek 50 TS ELISA reader (Merck) at an absorbance of 450 nm (x-axis) vs PDGF-BB concentration (y-axis), obtaining the formula y = 161.46x - 21.938, which was used to calculate the PDGF-BB values. The intra-assay coefficient of variation (CV) was less than 10% and the inter-assay CV was less than 12%. The detection limit was 1 pg/ml, with a standard curve range of 0.549-400 pg/ml.
Statistical analysisThe distribution of the variables was evaluated using graphical and numerical methods. The Shapiro-Wilk test was used to determine normality. Numerical variables were presented as mean ± standard deviation, as they showed a normal distribution. Statistical analysis was performed using the STATA version 17 statistical program for Windows (StataCorp LP, College Station, Texas, USA). Graphs were created using GraphPad Prism Version 8.
Ethical aspectsThis study was approved by the Ethics Committee of the Universidad Peruana Cayetano Heredia (Certificate E-043-09-23) and the Ethics Committee of the Hospital Cayetano Heredia (Certificate No. 160-2022). Pregnant women signed an informed consent form before the procedures of this study were carried out.
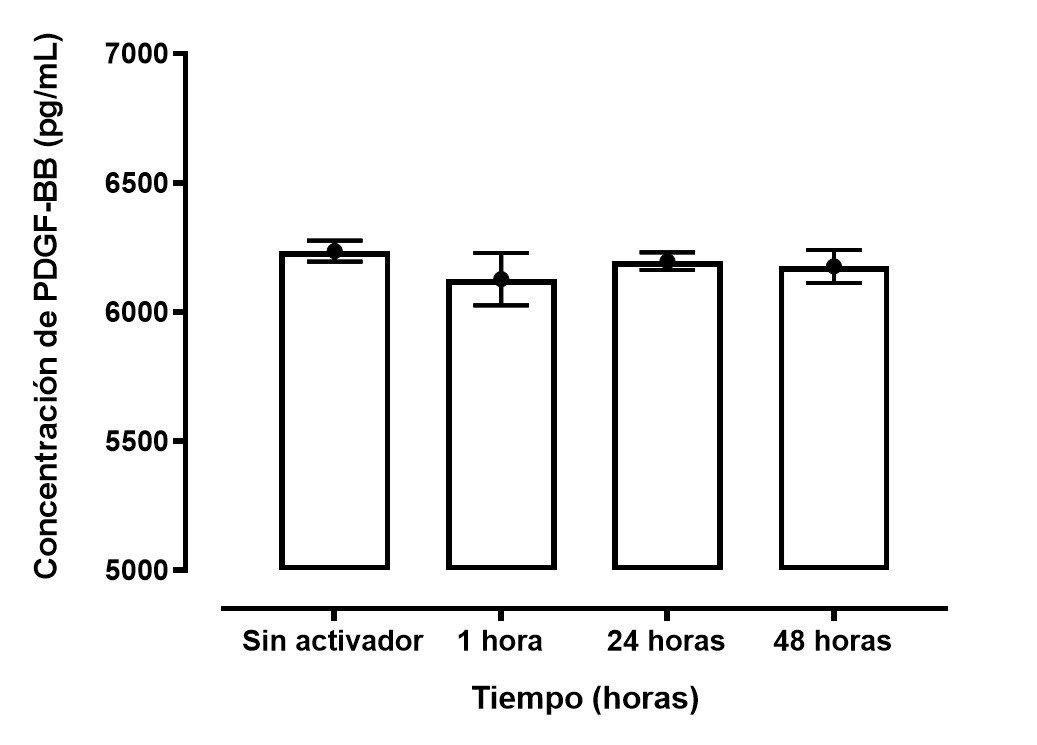
RESULTSA total of 6 umbilical cord blood samples were collected from term pregnant women, who had a mean age ± standard deviation (SD) of 22.1 ± 3.8. The mean (SD) platelet concentration post-centrifugation was higher than before centrifugation (617.2 ± 88.9 vs. 221.2 ± 42.3). The release of PDGF-BB was constant and sustained during the time periods measured at 1 hour, 24 hours, and 48 hours (6127.9 ± 101.6 pg/mL, 6197.5 ± 34 pg/mL, and 6176.8 ± 63.3 pg/mL, respectively). Additionally, a sample without 10% CaCl2 was added as a control, as shown in Table 1.
|
Characteristics |
Mean ± SD |
|---|---|
| Age (years) | 22.1 ± 3.8 |
| Platelets pre-centrifugation (103 uL) | 221.2 ± 42.3 |
| Platelets post-centrifugation (103 uL) | 617.2 ± 88.9 |
| PDGF-BB Concentration (pg/ml) | |
| Without activator | 6236.8 ± 40.5 |
| 1 hour | 6127.9 ± 101.6 |
| 24 hours | 6197.5 ± 34 |
| 48 hours | 6176.8 ± 63.3 |
PDGF-BB: Platelet-Derived Growth Factor Type BB.
SD: Standard deviation.
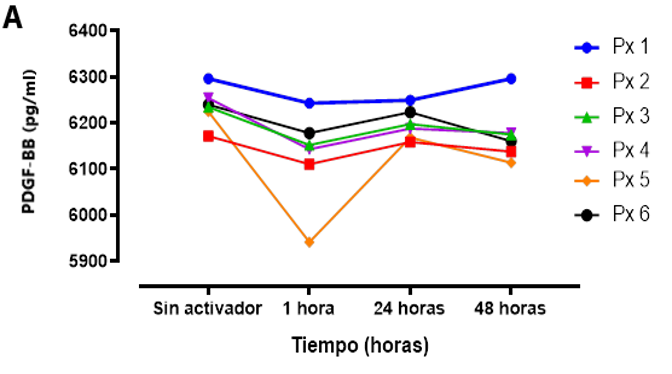
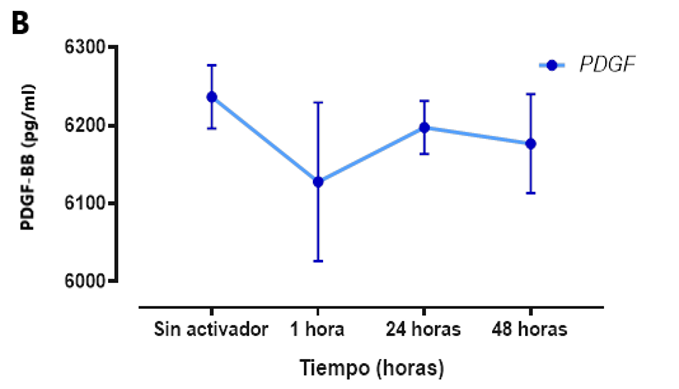
The concentration of PDGF-BB in the samples measured at specific time points was above 6000 pg/ml (Figure 3). The dynamics of PDGF-BB release were observed, which were rapidly induced but remained constant and sustained during the first hour, 24 hours, and 48 hours after activation. It is worth mentioning that the same trend was observed in the group that was not activated with Glu.Ca. In Figure 3 (A), the variability of PDGF-BB release for each sample is shown, while in (B), the variability is shown using the average release of PDGF-BB after 1 hour, 24 hours, and 48 hours post-activation.
Figure 2: PDGF-BB concentration obtained from PRP of umbilical cord blood measured at different time points (1 hour, 24 hours, and 48 hours)..
This study presents the first estimation of the kinetics of PDGF-BB release in PRP obtained from UC blood. The main finding was that this GF maintained a steady concentration during the first 48 hours after activation. Additionally, higher concentrations of PDGF-BB were observed compared to those reported in the literature for peripheral blood(16,17).
PRP is used as a source of growth factors, which play a crucial role in tissue regeneration(18). Various authors mention that the median concentrations of PDGF-BB in the blood of healthy subjects are approximately 4 ng/ml(19,20). However, GF concentrations can vary depending on the method and type of PRP obtained. Munawirah et al.(21) conducted a study to quantify PDGF-BB in PRP from peripheral blood using EDTA tubes and different centrifugation methods, obtaining average concentrations between 8330.86 pg/ml and 5206.75 pg/ml. Similarly, Amable et al.(22) observed that PRP activated with calcium chloride (CaCl2) and obtained in 3.2% citrate tubes showed PDGF-BB concentrations of 20.1 ± 10 ng/ml, similar to those reported by Lee et al.(16), who obtained a PDGF-BB concentration of 37.15 ± 1.62 ng/ml from activated PRP from peripheral blood. These variations can also be observed in the concentrations of PDGF-BB obtained from UC blood. Yan et al.(23) characterized PDGF-BB from platelet lysate of UC blood, obtaining a mean of 7.62 ± 1.29 ng/ml, while Murphy et al.(3) observed high concentrations of over 100,000 pg/ml for PDGF-AA/BB from PRP of peripheral and UC blood activated with calcium but lower values in those that were not activated. In addition, Buzzi et al.(13) showed PDGF values of 3233.2 (3461.7-4274.3) pg/ml, with collection through blood donation bags, findings similar to our study. The optimal conditions for GF release remain unresolved(24). The variation shown in our results compared to different studies could be based on many factors such as patient age and sex, the method of PRP preparation, platelet count, the preparation method, and the materials used for activation and measurement(25).
Most studies on the kinetics of growth factors have been conducted on PRP obtained from peripheral blood. Our results show constant and sustained values of PDGF-BB during the first 48 hours, with values above 5000 pg/ml, higher than those reported by Roh et al.(2), who found constant PDGF-BB values in PRP from peripheral blood during the first 7 days, with CaCl2 activation inducing values over 1000 pg/ml. Mariani et al.(26) also observed constant concentrations below 5000 pg/ml of PDGF-AA/BB for 168 hours. In contrast, Roffi et al.(27) showed high values released of PDGF-AA/BB at 1 hour of 27,714.68 (18,591.5-35,850.24) pg/ml and at 7 days of 31,670.63 pg/ml (18,617.58-80,462.27), likely due to the amount of blood collected for PRP preparation (150 ml). The incubation periods in this study were based on current knowledge about the initiation of angiogenic and osteogenic processes over days(2,28), thus our data showing sustained GF values could be fundamental in deciding the timing of PRP application. An important finding in our study is the observed PDGF-BB concentrations in PRP without stimulation, which were almost similar to those obtained by adding 10% CaCl2, possibly due to manual handling, temperature, and pressure applied to the platelet within the needle, which could also stimulate its release(29).
PDGF is a GF released from platelets during the blood coagulation process, involved in normal wound healing and tissue repair processes(30). It has four isoforms: A, B, C, and D(31). PDGF-BB is the most typical isoform, functioning in cell repair and proliferation, stimulating angiogenesis and collagen synthesis, playing an essential role in tissue healing(32). The Food and Drug Administration (FDA) considers this GF safe, with formulations approved for ulcer healing and bone regeneration(33). PRP injections, including different GFs (including PDGF-BB), have shown benefits in osteotendinous injuries, but limitations remain due to the lack of control over the amount and timing of administration(31). Therefore, this study specifically evaluated the kinetics of PDGF-BB to demonstrate the dynamics of its behavior over time.
LIMITATIONS AND STRENGTHS
Our study has limitations. Firstly, our experimental design only measured PDGF-BB concentrations at three time points, leaving the possibility that values may increase in subsequent days, as shown in some studies(2). Secondly, PDGF-BB was only measured at specific time points, without considering its depletion or degradation, which may occur due to denaturation, oxidation, or proteolysis, aspects not evaluated in this study(34). Thirdly, the differences observed in our PDGF-BB values compared to other reports could be influenced by different activation factors or the centrifugation method used in this study, affecting the kinetics. Fourthly, no direct assessment of the kinetics of PDGF-BB in PRP obtained from UC blood has been reported, so our results were compared with studies based on PRP obtained from peripheral blood. Fifthly, the collection (additive tubes) and transportation of samples to processing could have influenced the platelet concentration in terms of structure, exposure to degrading enzymes, and GF release(35). Finally, due to the number of samples obtained, only descriptive data were provided, without a more representative statistical analysis. However, the strength of this study is that it is the first to evaluate the kinetics of PDGF-BB using PRP obtained from UC blood, and these results could provide insights for future research in regenerative medicine.
In conclusion, our study shows that the release of PDGF-BB from PRP obtained from UC blood was induced rapidly and remained constant and sustained during the first 48 hours after activation, with concentrations above the normal range reported in the literature. UC blood could be an alternative for obtaining PRP, potentially useful for regenerative medicine due to its unique properties that could be therapeutically used for various ocular conditions, as an adjuvant to aid in skin wound healing, and joint regeneration processes.
Conflict of interest statement: The authors declare no conflict of interest.
This study is part of the thesis: Peralta A and Nisi A. Evaluation of the kinetics of the
release of platelet-derived growth factor (PDGF-BB) from platelet-rich plasma obtained from
umbilical cord blood [Thesis for the professional title of Pharmaceutical Chemist]. Lima:
Faculty of Science and Engineering, Universidad Peruana Cayetano Heredia; 2023.
Authorship contribution: PA, AP, and AN participated in the conceptualization,
investigation, methodology and statistics, resources, writing, and approval of the final
version. CL participated in the conceptualization, methodology and statistics, and approval
of the final version. CP and WB participated in the investigation and resource acquisition.
RP and JA participated in the critical review of the article and approval of the final
version.
Funding: The study was funded by the authors.
Received: February 15, 2024
Approved: May 20, 2024
Corresponding author: Pedro Aro
Address: Av. Honorio Delgado 430, San Martín de Porres. Lima, Perú.
Phone number: (01) 319-0000 - 980815956
E-mail: pedro.aro.g@upch.pe
Article published by the Journal of the faculty of Human Medicine of the Ricardo Palma University. It is an open access article, distributed under the terms of the Creatvie Commons license: Creative Commons Attribution 4.0 International, CC BY 4.0 (https://creativecommons.org/licenses/by/4.0/), that allows non-commercial use, distribution and reproduction in any medium, provided that the original work is duly cited. For commercial use, please contact revista.medicina@urp.edu.pe.