CLINIC CASE
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2024 - Universidad Ricardo Palma10.25176/RFMH.v24i2.6438
RADIOFREQUENCY ABLATION OF THYROID NODULES: A SUCCESSFUL CASE IN A PUBLIC HOSPITAL IN PERU
ABLACIÓN POR RADIOFRECUENCIA DE NÓDULOS TIROIDEOS; A PROPÓSITO DE UN CASO EXITOSO EN UN HOSPITAL PÚBLICO EN PERÚ
Enrique Bedoya-Ismodes
 1,2,a,b,
Erick Gonzales-Laguado
1,c,d,
Karem Portugal
1,2,e,f,
Nestor Juarez-Herrera
1,g
1,2,a,b,
Erick Gonzales-Laguado
1,c,d,
Karem Portugal
1,2,e,f,
Nestor Juarez-Herrera
1,g
1Hospital Santa Rosa, Lima, Perú
2Facultad De Medicina Humana, Universidad De San Martín De Porres, Lima, Perú
aMagister en Gerencia de Servicio de Salud
bResidente de Cirugía Oncológica
cMedico Cirujano Especialista en Cirugia de Cabeza y Cuello
dAsistente de Cirugia de Cabeza y Cuello
eMedico Cirujano Especialista en Oncologia Medica
fAsistente De Medicina Oncológica
gMedico Cirujano Especialista En Cirugia General Y Oncologica
ABSTRACT
The results are presented, suggesting the viability of radiofrequency ablation (RFA) as an effective
therapeutic strategy in the case of a 56-year-old woman with a benign thyroid nodule instead of
traditional surgery at a Public Hospital in Peru. The 6-month follow-up revealed a significant reduction
in the size of the nodule and a 70% reduction in volume; in addition to improved quality of life,
symptom improvement, and normal thyroid function. This case highlights the evolution in the treatment of
benign thyroid nodules, with RFA as a possible minimally invasive and safe option, offering a promising
alternative to conventional surgical interventions for the management of thyroid nodules, marking a
significant change in clinical practice. This is because it is the first hospital of the MINSA (Ministry
of Health) to perform such procedures, offering multiple treatment approaches for thyroid nodules: RFA,
transoral endoscopic thyroidectomy, conventional thyroidectomy, and active surveillance.
Keywords: Radiofrequency ablation, thyroid nodule, thyroid cancer, Hospital, RFA. (source: MeSH
NLM)
RESUMEN
Se expone los resultados que sugieren la viabilidad de la ablación con radiofrecuencia (ARF) como una
posible estrategia terapéutica efectiva en el caso de una mujer de 56 años con un nódulo tiroideo
benigno en lugar de la cirugía tradicional en un Hospital Público del Perú. El seguimiento a los 6 meses
reveló una reducción significativa en el tamaño del nódulo y reducción del 70% del volumen; además de
mejorar la calidad de vida, mejora en los síntomas y función tiroidea normal. Este caso destaca la
evolución en el tratamiento de nódulos tiroideos benignos, con la ARF como una posible opción
mínimamente invasiva y segura, la cual se ofrece una alternativa prometedora a las intervenciones
quirúrgicas convencionales para el manejo de nódulos tiroideos, marcando un cambio significativo en la
práctica clínica, ya que es el primer hospital del MINSA (Ministerio de Salud) en realizar este tipo de
procedimientos y que ofrece múltiples enfoques de tratamiento de nódulos tiroideos: ARF, tiroidectomía
endoscópica transoral, tiroidectomía convencional y vigilancia activa.
Palabras clave: Ablación por Radiofrecuencia, Nódulo Tiroideo, Cáncer de Tiroides,
Hospital.(fuente: DeCS-BIREME)
INTRODUCTION
Thyroid radiofrequency ablation (RFA) is a medical intervention designed to address benign thyroid
nodules (BTN), utilizing radiofrequency energy to selectively destroy abnormal cells while preserving
the surrounding tissue (1, 2).
In the RFA procedure, alternating current with a variable frequency between 200 and 1200 kHz is used,
thereby generating localized thermal energy and raising the temperature to a range of 50 to 100 °C
(1). This results in both direct and indirect heating. The area of direct
heating, close to the electrode, has a high current density that generates heat through friction,
causing immediate damage to the tumoral tissue, especially in regions near the electrode. On the other
hand, conduction heat propagates to more distant tumoral tissues through thermal conduction (1) (Figure 1).
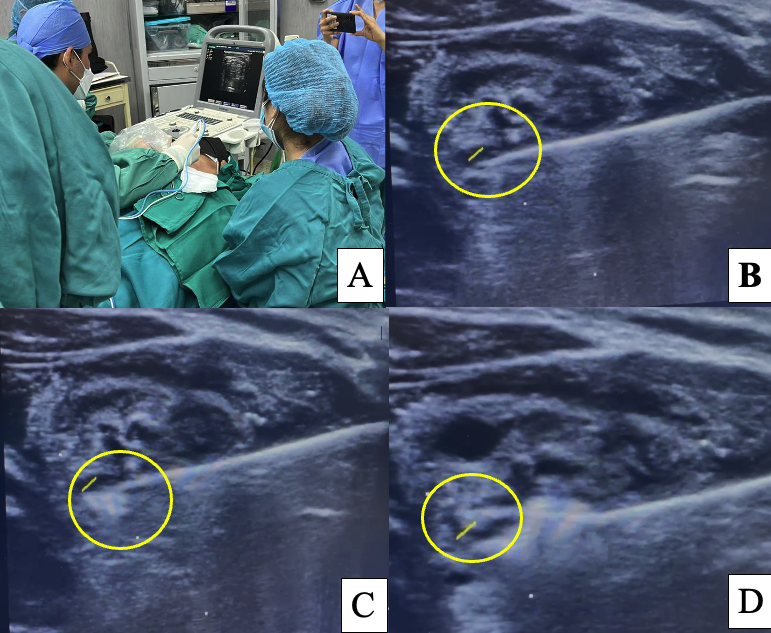
Figure 1. Ultrasound-guided Radiofrequency Ablation (RFA) Procedure in the surgical center of Hospital Santa Rosa, Lima, Peru.
The tip of the electrode is inserted into the deepest part of the nodule and gradually withdrawn towards
the superficial layers, ensuring a margin of normal thyroid tissue. Five percent dextrose is applied for
hydrodissection. In some cases, a saline solution can be used as a buffer to protect adjacent structures
(1).
RFA is an innovative minimally invasive therapeutic option in the treatment of benign thyroid nodules
and selected cases of low-risk thyroid cancer, preserving thyroid function without the need for
replacement therapy. Additionally, the absence of scars contributes to a higher level of patient
satisfaction (3 - 5).
We aim to present the results supporting the feasibility of radiofrequency ablation as a potential
effective therapeutic strategy to improve the quality of life for patients with thyroid nodules,
offering a promising alternative to conventional surgical interventions (1, 5, 6).
In this regard, we present Hospital Santa Rosa located in Lima, Peru, as the first hospital within the
MINSA network to perform this type of procedure, becoming the first public hospital to offer multiple
treatment approaches for thyroid nodules: RFA, transoral endoscopic thyroidectomy, conventional
thyroidectomy, and active surveillance.
Case Report
A 56-year-old female patient from Lima with a history of glaucoma, hypertension, and prediabetes. She
presents a 4-year clinical history characterized by the progressive growth of a nodular mass in the
right thyroid lobe.
In May 2022, the patient sought medical attention at the oncology service, head, and neck clinic of HSR
due to the increase in the size of the right thyroid nodule. A thyroid ultrasound was performed,
revealing a nodule in the right thyroid lobe with dimensions of 50.87 x 39.89 x 34.54 mm, a volume of
36.8 ml, and a thyroid profile within the normal range (Figure 2A).
Subsequently, a Fine Needle Aspiration Biopsy (FNAB) was performed, with a pathological result
classifying the nodule as Bethesda II (Benign). Initially, surgical treatment (thyroidectomy) was
offered, but the patient declined surgery.
In October of the same year, the patient returned to the oncology service at the head and neck clinic of
HSR for reevaluation, without significant clinical changes or alterations in ultrasound studies. The
option of undergoing RFA was explained and offered to her, detailing the benefits and main
characteristics of the procedure.
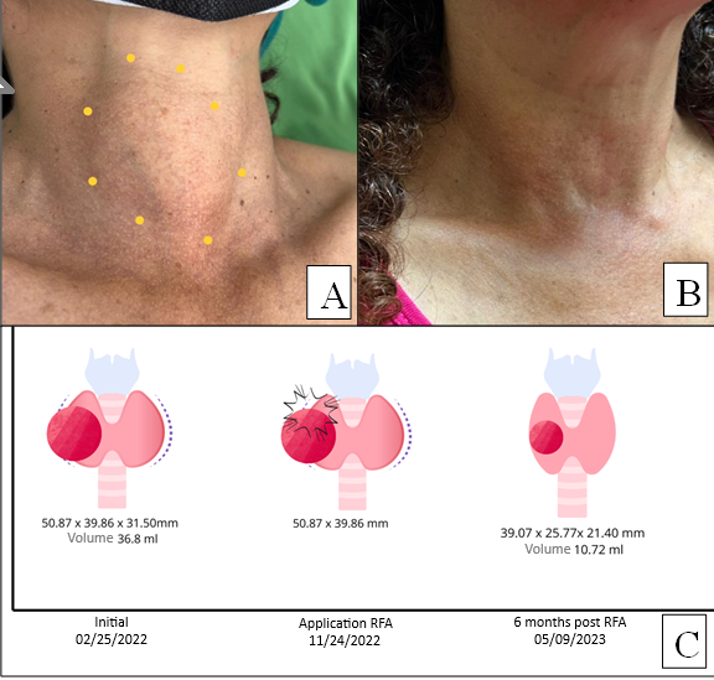
Figure 2. Clinical and Ultrasound Changes in Thyroid Nodule Before and 6 Months After Radiofrequency Ablation.
The RFA procedure was successfully performed on an outpatient basis in November 2022. The patient
tolerated it well and experienced no complications during the procedure. Aseptic and antiseptic measures
were taken, and 2% lidocaine without epinephrine was infiltrated into the anterior cervical region. The
thyroid nodule was identified via ultrasound, hydrodissection was performed with 5% dextrose, and RFA
was then carried out. RFA is an outpatient procedure performed in an operating room under local
anesthesia, using lidocaine at the puncture site and thyroid capsule. During the procedure, the patient
is placed in a supine position with neck extension, while the operator, positioned at the patient's
head, evaluates the nodule's position using ultrasound. A high-frequency linear probe is used to select
the most appropriate approach and to monitor and guide the ablation procedure. All of this is done under
strict aseptic conditions, emphasizing the safety and control of the procedure (Figure 1).
At the 6-month follow-up, ultrasound revealed a notable reduction in the nodule size to 39.07 x 21.41 x
25.77 mm (volume 10.72 ml), (Figure 2C) with positive results, symptom reduction, and a thyroid profile
within normal limits.
Discussion
This case report highlights the evolution in the treatment of benign thyroid nodules (BTN) traditionally
managed with conventional methods such as thyroidectomy or hemithyroidectomy (1). In the last decade, minimally invasive techniques like radiofrequency
ablation (RFA) have been proposed, emerging as a percutaneous minimally invasive option to treat benign
nodules of the thyroid and parathyroid glands. Initially considered an alternative to surgery, RFA has
gained importance, demonstrating its efficacy in both solid and partially cystic nodules, including
cases of differentiated thyroid cancer (5 - 7).
It has been proven that RFA effectively reduces nodule volume with low complication rates and
significant improvements in related symptoms, as observed in our case (5).
This approach avoids the adverse effects of surgery, such as the risk of bilateral recurrent laryngeal
nerve injury, hypocalcemia, hypoparathyroidism, and the need for hormone replacement due to resection
(3 - 9).
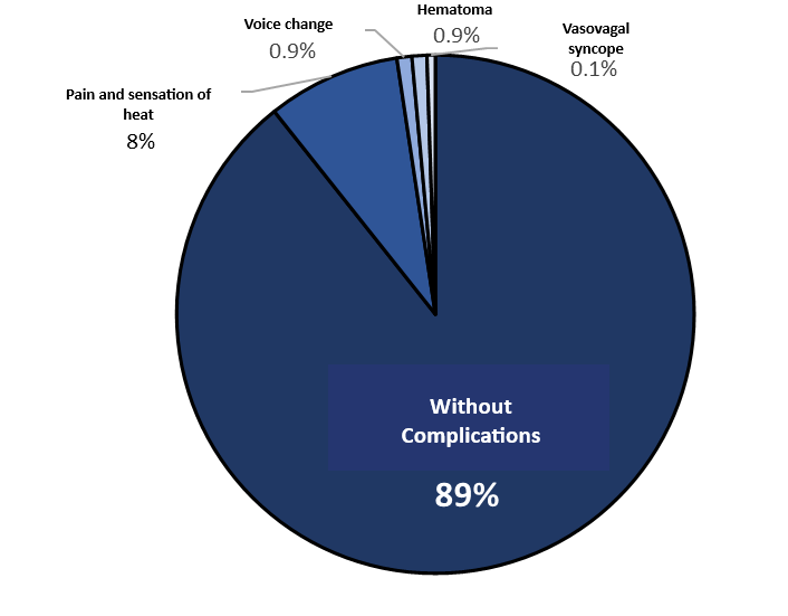
In a systematic review conducted by Wang et al. in 2017, which aimed to examine the safety of RFA as a
treatment method for benign thyroid nodules, it was found that out of 3,409 patients, 89% did not
experience complications, while 8% reported pain and a sensation of heat, 0.9% experienced voice
changes, 0.9% had hematoma, 0.1% had a vasovagal syncope, and less than 0.1% had other complications.
This indicates that RFA is a procedure with a broad range of safety (3, 10) (Figure 3).
Thyroid nodules subjected to thermal ablation should undergo regular follow-up through ultrasound and
clinical examinations. Ultrasound is established as the most reliable method for monitoring the
progression of treated nodules over time, including measurements of size, volume, and vascularization,
as well as the evaluation of cosmetic scores and symptoms. The effectiveness of the treatment is
assessed by the volume reduction rate (VRR), which is progressive, with the final reduction typically
evident at an average of 12 months (1, 4, 11).
CONCLUSION
In conclusion, this report suggests the RFA technique as an effective and minimally invasive alternative
to traditional surgery for the treatment of benign thyroid nodules. Through the case of a 56-year-old
female patient, within just 6 months, the thyroid nodule reduced its volume from 36.8 ml to 10.72 ml,
corresponding to a Volume Reduction Rate (VRR) of 70.85%. Compressive symptoms are no longer present,
the thyroid profile is normal, the thyroid nodule is not visually evident, and the patient's
satisfaction level is high. Literature has demonstrated that volume reduction is progressive, with the
final reduction typically evident at an average of 12 months.
This approach represents a significant change in clinical practice at Hospital Santa Rosa and other
public hospitals in Peru, highlighting the multiple treatment approaches for thyroid nodules: RFA,
transoral endoscopic thyroidectomy, conventional thyroidectomy, and active surveillance. The safety of
the procedure, combined with its outpatient nature and ultrasound guidance, underscores RFA as a
valuable and safe option for the treatment of thyroid nodules, marking a significant milestone in the
care of these cases in hospital settings.
Authorship contributions:
EBI, EGL, PK, and NJH participated in the conceptualization, data curation, formal analysis,
investigation, methodology, supervision, validation, original draft writing, review and
editing, and approval of the final version.
Financing:
Self-funded
Declaration of conflict of interest:
The authors declare no conflict of interest in the presentation of this manuscript.
Recevied:
January 11, 2024
Approved:
March 31, 2024
Correspondence author:
Enrique Oswaldo Bedoya Ismodes.
Address:
Alameda del Corregidor 1531, La Molina 15024.
Phone:
982508211
E-mail:
enrique_bedoya@usmp.pe
Article published by the Journal of the faculty of Human Medicine of the Ricardo Palma University. It is an open access article, distributed under the terms of the Creatvie Commons license: Creative Commons Attribution 4.0 International, CC BY 4.0 (https://creativecommons.org/licenses/by/4.0/), that allows non-commercial use, distribution and reproduction in any medium, provided that the original work is duly cited. For commercial use, please contact revista.medicina@urp.edu.pe.
BIBLIOGRAPHIC REFERENCES
