ORIGINAL ARTICLE
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2024 - Universidad Ricardo Palma10.25176/RFMH.v24i2.6550
BIOMEDICAL ANTHROPOMETRIC EVALUATION AND CONCEPTUAL MECHANICAL DESIGN OF ROBOTIC SYSTEM FOR LOWER LIMBS PASSIVE-REHABILITATION ON POST-STROKE PATIENTS
FEVALUACIÓN ANTROPOMÉTRICA BIOMÉDICA Y DISEÑO MECÁNICO CONCEPTUAL DE UN SISTEMA ROBÓTICO PARA LA REHABILITACIÓN PASIVA DE MIEMBROS INFERIORES EN PACIENTES POST-ACCIDENTE CEREBROVASCULAR
Cesar Martel Cervantes
 1
1
Carol Sandoval
1
Ricardo Palomares
1
Jeanette Borja Arroyo
2
Margarita Murillo Manrique
1
Jose Cornejo
1
1Grupo de Investigación en Robótica y Mecatrónica Avanzada (GI-ROMA), Universidad Ricardo Palma,
Lima, Peru.
2 Hospital Edgardo Rebagliati Martins, Lima, Peru.
ABSTRACT
Background: Cerebrovascular accident (CVA) is one of the main causes of permanent disability, as
it can cause serious brain injuries with significant physical consequences, limiting the ability to
perform daily activities.
Objective: This research aimed to design a robotic system of passive-continuous movement for the
rehabilitation of lower limbs in adult patients with stroke, thus improving the chances of recovery of
their walking mobility.
Methodology: Modeling and simulation of the robotic system using Computer Aided Design (CAD),
using the engineering software Autodesk Inventor Professional 2023.
Results: The initial and final positions of the robotic system were obtained, as well as the
simulation of passive-continuous movement.
Conclusions: Taking precise measurements of a patient maximizes the possibility of implementing a
functional prototype that contributes to the rehabilitation process.
Keywords: robotics, rehabilitation, lower limbs, design, cerebrovascular accident, simulation
(source: MeSH NLM)
RESUMEN
Antecedentes: El accidente cerebrovascular (ACV) es una de las principales causas de discapacidad
permanente, ya que puede provocar lesiones cerebrales graves con secuelas físicas significativas,
limitando la capacidad de realizar actividades diarias.
Objetivo: Esta investigación tuvo como objetivo diseñar un sistema robótico de movimiento
pasivo-continuo para la rehabilitación de miembros inferiores en pacientes adultos con ACV, mejorando
así las probabilidades de recuperación de su movilidad de marcha.
Metodología: Se llevó a cabo el modelado y simulación del sistema robótico mediante Diseño
Asistido por Computadora (CAD), utilizando el software de ingeniería Autodesk Inventor Professional
2023.
Resultados: Se obtuvieron las posiciones iniciales y finales del sistema robótico, así como la
simulación de movimiento pasivo-continuo.
Conclusiones: La toma de medidas precisas de un paciente maximiza la posibilidad de implementar
un prototipo funcional que contribuya en el proceso de rehabilitación.
Palabras clave: robótica, rehabilitación, miembros inferiores, diseño, accidente cerebro
vascular, simulación.
(fuente: DeCS- BIREME)
1. INTRODUCTION
In Peru, according to the 2017 Specialized Disability Survey conducted by the Instituto Nacional de
Estadística e Informática (INEI), 10.3% of the population, approximately 3,209,261 people, have some
form of disability [1]. Among these, a total of 10,570 cases of patients
with stroke were recorded [2]. It is estimated that 60% of people
hospitalized due to stroke suffer from disabling sequelae, and only 20% of those affected complete
physical rehabilitation programs [4]. According to the 2019 INEI data, 88.6%
of the total population with some type of disability did not receive treatment or rehabilitation
therapy, while only 11.4% managed to access some form of care in this regard [5]. This disparity can be partly attributed to the lack of utilization of
rehabilitation technology in Peru, due to economic factors and lack of awareness about the existence of
these devices as part of physical rehabilitation therapies.
Stroke can be prevented by leading a healthy lifestyle and, if it occurs, can be effectively treated if
the patient is taken to a hospital emergency room as soon as possible after presenting the first signs,
at which point the chances of recovery are high [6]. For the aforementioned
reasons, the design of a continuous passive motion robotic system for the rehabilitation of lower limbs
in adult patients affected by stroke is proposed. This system aims to facilitate and maximize the
recovery of motor functions of the lower extremities, both at home and in hospital settings, with
monitoring and follow-up by the rehabilitation physician. Currently, various studies have been developed
to address the diverse mobility problems of the lower limbs, including, for example, the development of
systems for gait assistance [6], treatment of motor disabilities caused by
cerebral palsy [8], and the development of control applications for
exoskeletal systems [8]. However, the first models of exoskeletons emerged
in the 1960s in the laboratories of Cornell University [9].
Yang's structure represents one of the first documented attempts with exoskeletal characteristics, whose
primary objective was to increase power in walking rhythm and jumping [10].
Another version of this type of exoskeleton was implemented with direct current motors. However, the
motor, power system (battery), and computational technology of the time greatly limited the portability
of the device [11].
In Spain, at the Universidad Politécnica de Catalunya, a design of an active knee-ankle orthosis was
presented [12]. This project focuses on assisting and recovering patients
with spinal cord injury, whose condition often leaves them without mobility in approximately 80% of
their body. In Latin America, exoskeletons have been developed for the rehabilitation of arms as well as
legs. In the field of arm rehabilitation, for example, advances have been made with exoskeletons
offering up to four degrees of freedom, adapted to the anthropometry of Mexican patients through optimal
conceptual design [13]. These exoskeletons focus on the rotation movement
of the humerus, flexion and extension of the elbow [14], pronation, and
supination of the hand [15]. In the case of leg rehabilitation, systems
with two degrees of freedom for ankle and knee therapies have been developed, including the use of
force, speed, and position sensors [16], as well as designs exclusive for
knee flexion-extension [17]. In this sense, the application of technology
in physical rehabilitation improves patient independence when attending their therapies, as demonstrated
by research [18].
In conclusion, the development of the project represents a significant advancement in the implementation
of rehabilitation equipment that improves the physical condition of patients with gait limitations due
to stroke, allowing them to be more independent in their daily activities. In the future, the research
aims to implement the lower limb robotic system, providing patients the opportunity to recover an
essential component of their function and autonomy under the supervision of the rehabilitation
physician.
2. METHODOLOGY
2.1. Biomechanical analysis of lower limbs
This project focuses on the biomechanical analysis of the lower extremities, which includes the knee and
foot as shown in Figure 1, with the purpose of designing a robotic system for the rehabilitation of
stroke patients. The movements and functions of the joints are examined in different contexts to
identify specific rehabilitation needs. The critical biomechanical factors to consider in the design of
an exoskeleton are the degrees of freedom and movements [19], which are
fundamental for the development of computer-aided design (CAD) modeling that facilitates the recovery of
motor function in patients who have experienced a stroke.
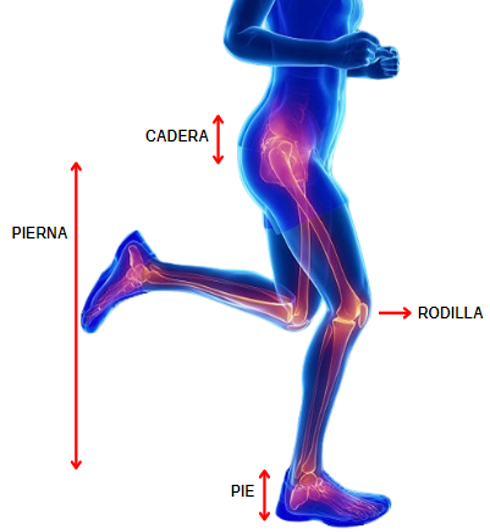
Figure 1. Anatomy of the lower limb.
Source: Adapted from https://www.goconqr.com/es/p/26439765?dont_count=true&frame=true&fs=true
The joints of the lower limb are illustrated, including the hip, knee, and ankle [20], represented by red circles. Lines connect these joints, showing the movement trajectories during the rehabilitation process [21]. It can be observed how the system's design allows for multidirectional movements and personalized adjustments, offering a wide range of exercises to improve mobility and muscle strength in patients with lower limb dysfunction, as shown in Figure 2.
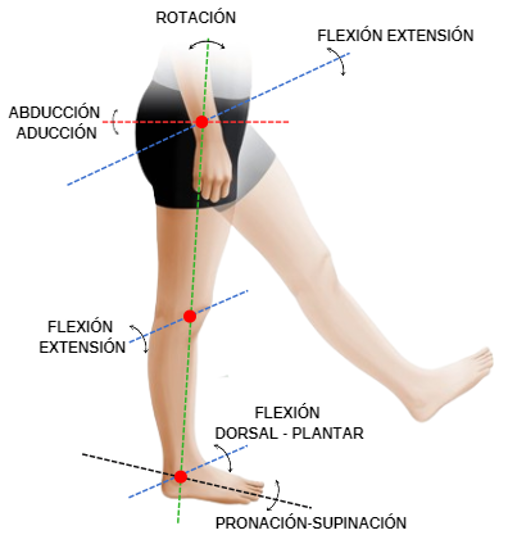
Figure 2. Movement of lower limb joints.
Source: Adapted fromhttps://www.kenhub.com/es/library/anatomia-es/tipos-de-movimientos-del-cuerpo-humano
According to Table 1, the degrees of biomechanical movement in the knee and ankle joints [22] allow the design of robotic rehabilitation systems that can provide personalized and specific therapies for each patient. The ability to adjust the resistance and speed of movement based on the individual needs of each patient [23]is essential for optimizing rehabilitation outcomes and promoting effective recovery of motor function in the lower limbs.
|
Joint |
Movement |
Degrees |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
Knee |
Extension – Flexion |
0° a 120° |
|||||||||
|
Ankle |
Plantar – Dorsal Flexion |
-40° a 20° |
|||||||||
|
Supination – Pronation |
-35° a 15° |
Taken from “Basic Biomechanics of the Musculoskeletal System” (Nordin, 2004).
The measurement of the lower limb was performed by dividing it into L1, L2, and L3 as shown in Figure 3, based on the anatomy and individual proportions of the patient [24]. The correct implementation of these anthropometric measurements ensures proper biomechanical alignment and balanced load distribution during the rehabilitation process, which is essential for maximizing the effectiveness and safety of the treatment. This allows for optimal adjustment to create the CAD prototype design of the lower limb robotic rehabilitation system.
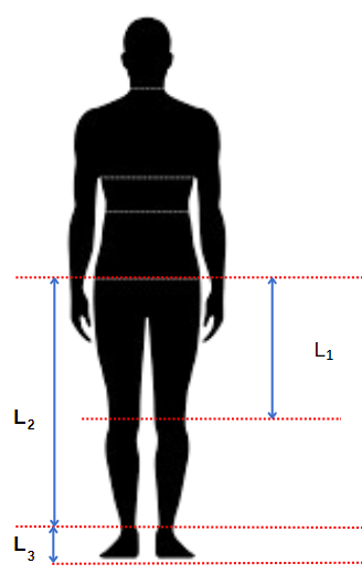
Figure 3. Anthropometric measurements of the lower limb.
Source: Adapted from https://depositphotos.com/es/vectors/icono-cuerpo-humano.html
2.2 3D mechanical design of the robotic system
The present mechanical design of the robotic system is based on the patient’s anthropometric measurements, focusing primarily on the biomechanics of each joint. Its objective is to carry out adequate rehabilitation of the knee and ankle as a result of a stroke [25]. Autodesk Inventor Professional 2023 software was used to design the parts of the structure, which is divided into a leg and foot support, similar to the exoskeleton [18], where the obtained results are within the permitted resistance limits for material validation and selection. Additionally, the base of the device is composed of a support and a rail system, as shown in Figure 4. This device is planned to be prototyped using 3D printing in the next stage of the project [26].

Figure 4. CAD design of the knee and ankle system.
Source: Created in Autodesk Inventor Professional 2023.
2.3 Kinematic structure of the lower limb
The objective of kinematics in a lower limb robotic system is to analyze the movement capability through the position and orientation with joint coordinate values [27]. Figure 5 shows the geometric representation of the patient’s lower limb.
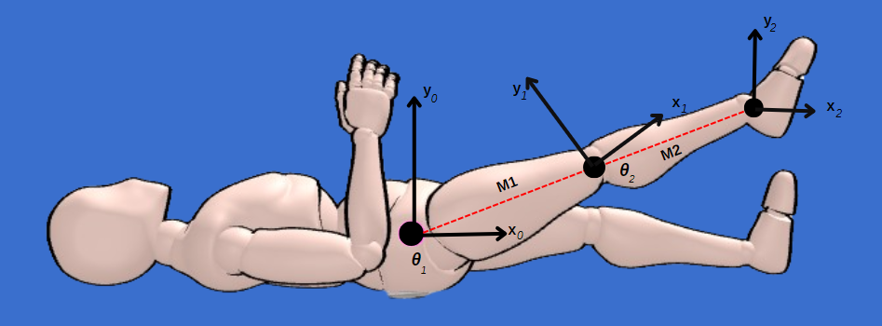
Figure 5. Kinematic structure of the lower limb.
Source: Elaborado en Just Sketch software.
Table 2 shows the geometric parameters of the lower limb according to the Denavit-Hartenberg (D-H) convention based on the reference systems and dimensions in Figure 5 [28].
|
Link i |
ai |
αi |
di |
Ɵi |
|||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
1 |
M1 |
0 |
0 |
Ɵ1 |
|||||||||||||||
|
2 |
M2 |
0 |
0 |
Ɵ2 |
Where:
i = represents the joint number
ai =distance along the xi axis
αi = distance between the zi and zi+1 axes
di = distance between the zi axes
Ɵi = angle between the xi y xi+1axes
The direct kinematic model allows calculating the position and orientation of the leg based on its joint angles. Therefore, it is necessary to calculate the homogeneous transformation matrix Ai for each joint, as represented in equation 1.

By substituting the joint parameters from Table 2 into equation 1, the following matrices are obtained:
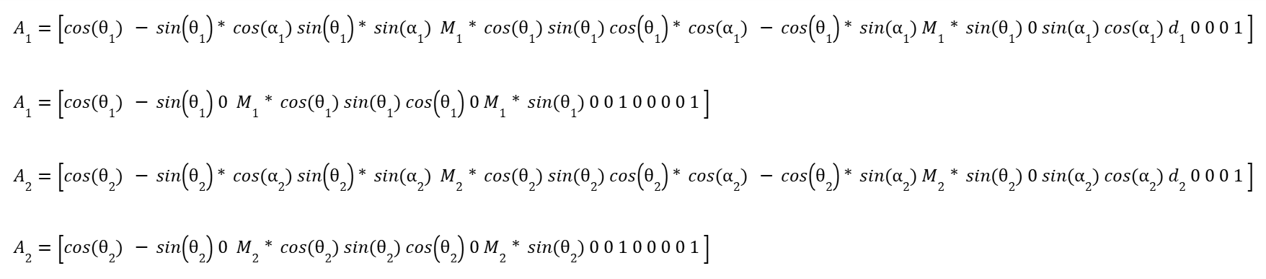
To obtain the direct kinematic model (position and orientation of the end) of the lower limb, it is necessary to multiply the matrices A1 and A2. Therefore, the homogeneous transformation matrix representing the position and orientation is represented in equation 2.

3. RESULTS
In the present research, the anthropometric data of a 40-year-old patient were analyzed, as shown in
Table 3, with lower limb limitations due to a stroke, a height of 170 cm, and a weight of 90 kg.
|
Limb |
Dimension (cm) |
||||||
|---|---|---|---|---|---|---|---|
|
Thigh |
43.01 |
||||||
|
Leg |
41.99 |
||||||
|
Foot |
6.63 |
The simulation results conducted in Autodesk Inventor Professional 2023 software, as shown in Figure 6, indicate that the robotic system meets the functional requirements for the rehabilitation and improvement of lower limb spasticity in stroke patients. The maximum flexion movements achieved (80° in the hip, 40° in the knee, and 20° in the ankle) are within the established therapeutic ranges, suggesting that the device can be effective in improving the degrees of movement in these patients, as assessed by the Modified Ashworth Scale [29].
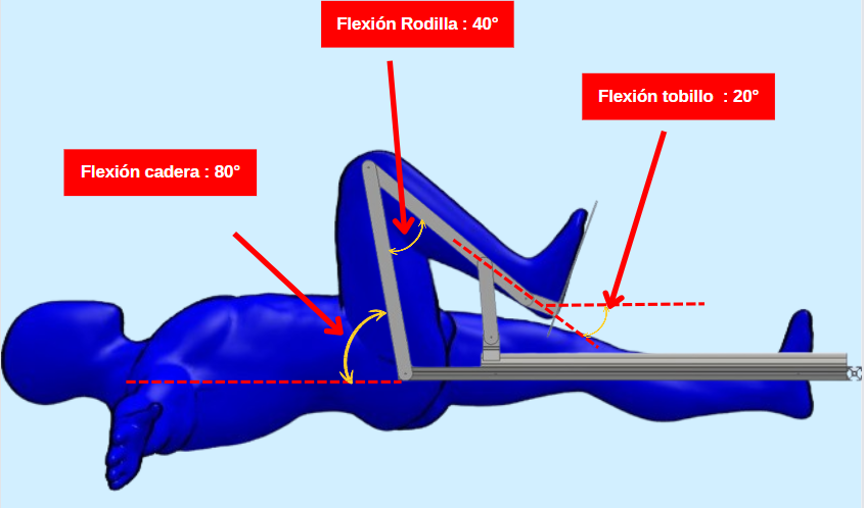
Figure 6. Simulation of the robotic system in flexion.
Source: Created in Autodesk Inventor Professional 2023.
For knee extension, the system successfully reached 180°, representing full extension. This range is crucial for facilitating natural movements and daily activities such as walking, standing up, and sitting down. The simulation showed that the knee mechanism can support the load without compromising stability, which is essential for effective rehabilitation. The precision in the simulation suggests that the system can replicate physiological movements with high fidelity, which is essential to avoid injuries and maximize therapy effectiveness. Additionally, the system's stability under maximum extension conditions ensures that patients can use it safely during prolonged rehabilitation sessions.
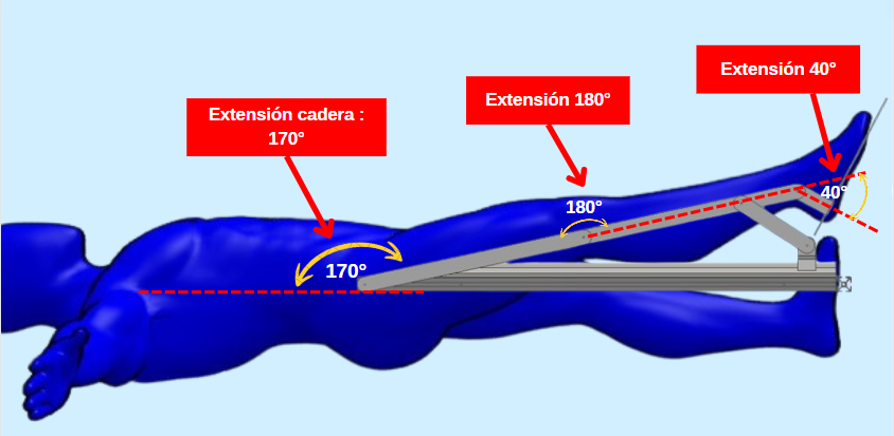
Figure 7. Simulation of the robotic system in extension
Source: Created in Autodesk Inventor Professional 2023.
The maximum extension angles achieved in the hip (170°), knee (180°), and ankle (40°), as shown in Table 4, are adequate to facilitate comprehensive functional recovery. These results support the use of this system as a potentially valuable tool in physical rehabilitation programs, contributing to improved quality of life for patients.
|
Limb |
Figure 7 |
Figure 8 |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
Hip |
80° |
170° |
|||||||||
|
Ankle |
40° |
180° |
|||||||||
|
Tobillo |
20° |
40° |
The precision in the simulation suggests that the system can replicate physiological movements with high fidelity, which is essential to avoid injuries and maximize therapy effectiveness.
4. CONCLUSIONS
This research demonstrates that the lower limb medical robotic system [31]
has been designed with biomechanical principles and simulated using the Denavit-Hartenberg (D-H)
algorithm, showing its potential to be a valuable tool in the rehabilitation of stroke patients by
providing knee and ankle movements essential for functional recovery. Additionally, the homogeneous
transformation matrices enable the creation of displacement graphs and simulations of leg movement,
providing better understanding and control of the rehabilitation process.
The extension and flexion angles achieved by the system are adequate to facilitate comprehensive
recovery. The system's ability to maintain these angles stably and controlled ensures that patients can
perform the necessary rehabilitation exercises without risk of injury, which is essential for safe and
effective therapy, thereby significantly improving the quality of life for stroke patients.
The results obtained not only confirm the conceptualization of the system's technical feasibility but
also open the possibility of developing real prototypes and evaluating them in clinical settings.
Moreover, this project has the potential to be used in future space missions where lower limb
rehabilitation is required, as muscle deterioration occurs in low-gravity environments [31]. As future work, it is proposed to implement and test the prototype,
conducting spasticity evaluations on the Modified Ashworth Scale before and after using the device
in a group of stroke patients to validate its in-situ effectiveness and optimize the design to an
ergonomic model. The next stage of the project, which will involve use in humans, will have the
approval of the Ethics Committee.
Authorship contributions:
C.M.C. and C.S. participated in the conceptualization, research, methodology, data analysis
and interpretation, resources, and writing of the original draft; J.B.A. participated in
clinical supervision and application of results; R.P., M.M.M., and J.C. participated in
technical supervision and advice, data analysis and interpretation, writing of the article,
and critical revision of the article.
Founding:
This article is the product of the first phase of the research project "Design and
Simulation of a Continuous Passive Motion Robotic System for the Rehabilitation of Lower
Limbs in Adult Patients with Hemiplegia Due to Cerebrovascular Accidents (CVA)" approved by
University Council Agreement No. 182-2024 and funded by the Vice-Rectorate for Research of
Universidad Ricardo Palma.
Declaration of conflict of interest:
The authors declare no conflict of interest.
Received:
May 15, 2024
Approved:
June 08, 2024
Correspondence author:
Carol Sandoval
Address:
Av. Alfredo Benavides 5440, Santiago de Surco 15039, Lima-Peru.
Phone:
(+51) 999661222
E-mail:
keiko.sandoval@urp.edu.pe
Article published by the Journal of the faculty of Human Medicine of the Ricardo Palma University. It is an open access article, distributed under the terms of the Creatvie Commons license: Creative Commons Attribution 4.0 International, CC BY 4.0 (https://creativecommons.org/licenses/by/4.0/), that allows non-commercial use, distribution and reproduction in any medium, provided that the original work is duly cited. For commercial use, please contact revista.medicina@urp.edu.pe.
REFERENCIAS BIBLIOGRÁFICAS
