ORIGINAL ARTICLE
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2024 - Universidad Ricardo Palma10.25176/RFMH.v24i3.6625
QUALITY OF LIFE IN PATIENTS WITH TYPE 2 DIABETES MELLITUS
CALIDAD DE VIDA EN PACIENTES CON DIABETES MELLITUS TIPO 2
Nicole Solange Cadenillas-Maguiña
 1,a
1,a
Mayra Alejandra Rosas-Castillo
1,a
Marisa Esperanza Morillas
2,b
Evanilda Souza de Santana Carvalho
3,c
Kattia Ochoa-Vigo
2,c
1 DE JESUS UROMEDIC-Centro Especializado en Urologia, Barranca, Región Lima-Perú.
2 Universidad Nacional de Barranca, Barranca, Región Lima-Perú.
3 Universidade Estadual de Feira de Santana, Feira de Santana, Bahia-Brasil.
a Enfermera Asistencial.
b Magister en Psicología.
c Doctora en Enfermería.
ABSTRACT
Introduction: Type 2 diabetes mellitus in the Americas affects approximately 62 million people,
recognized as the most common chronic disease in the countries. It is estimated that by 2030, population
growth, aging, urbanization and changes in lifestyles will lead to a 54% increase in diabetes, with a
significant impact on quality of life.
Objective: Determine the level of quality of life of patients with type 2 diabetes mellitus,
Province of Barranca, Lima-Peru Region.
Methods: Observational study and descriptive design. The population was 242 patients attending a
public hospital, in the province of Barranca, with a random sample of 144 patients. Data collection was
carried out in the second quarter of 2021, through interviews using the WHOQOL-BREF questionnaire. Data
analysis was carried out with SPSS v.24 software.
Results: 69% of patients were women, aged between 40-64 years and an average of 58 years. The
quality of life was of a medium level (86%), with the social dimension being valued at a high level
(74%), while the physical dimension was valued at a low level (64%). When analyzed by sex, an average
quality of life predominated in both, and when grouped by age, those over 65 years of age rated a low
quality of life (29%).
Conclusions: Patients with type 2 diabetes mellitus presented a medium-level quality of life,
with the physical dimension valued at a low level, while the psychological and environmental dimensions
showed a medium level.
Keywords: diabetes mellitus, outpatient care, quality of life, nursing. (Source: MeSH – NLM)
RESUMEN
Introducción: La diabetes mellitus tipo 2 en las Américas afecta aproximadamente a 62 millones de
personas, reconocida como la enfermedad crónica más común en los países. Se estima que al 2030, el
crecimiento de la población, envejecimiento, urbanización y los cambios en estilos de vida conducirían a
un incremento de 54% de la diabetes, con impacto importante en la calidad de vida.
Objetivo: Determinar el nivel de calidad de vida de pacientes con diabetes mellitus tipo 2,
Provincia de Barranca, Región Lima-Perú.
Métodos: Estudio observacional y diseño descriptivo. La población fue de 242 pacientes asistentes
a un hospital público, en la provincia de Barranca, con una muestra aleatoria de 144 pacientes. La
recolección de datos se realizó el segundo trimestre-2021, mediante entrevistas utilizando el
cuestionario WHOQOL-BREF. El análisis de datos se efectuó con el software SPSS v.24.
Resultados: El 69% de pacientes era de mujer, con edades entre 40-64 años y una media de 58 años.
La calidad de vida fue de nivel medio (86%), valorándose la dimensión social en nivel alto (74%),
mientras que la física fue valorada con nivel bajo (64%). Al analizar por sexo, en ambos predominó una
calidad de vida media, y al agrupar por edad, los mayores de 65 años calificaron en una calidad de vida
baja (29%).
Conclusiones: Los pacientes con diabetes mellitus tipo 2 presentaron una calidad de vida de nivel
medio, siendo la dimensión física valorada con nivel bajo, mientras que la psicológica y ambiental
mostraron un nivel medio.
Palabras clave: diabetes mellitus, atención ambulatoria, calidad de vida, enfermería. (Fuente:
DeCS – BIREME)
INTRODUCTION
Diabetes mellitus (DM) is a chronic disease of global scope that continues to increase alarmingly, affecting millions of people worldwide, due to changes in lifestyles, the increase in obesity, together with population aging and urbanization(1). Alqurashi et al.(2) reported in their study that 30% of the population had diabetes, with a notable difference in prevalence between men and women, with a greater impact on men (34.1%).
In developed countries, DM affects older people, whereas in developing countries, the incidence increases among middle-aged people. This demographic difference may persist in the future(1), representing a public health problem for all countries, due to the high costs of treating its long-term complications(3,4).
In Latin America, the situation is also worrying, with a significant increase in the prevalence of type 2 diabetes and shocking figures of associated mortality. Between 2010 and 2020, 601,521 deaths related to DM were registered in Brazil and strongly associated in places with worse social indicators(4); a recent study in Brazil indicates an overall prevalence of 24%(5). In Mexico, the prevalence was 18.3%, and 22.1% of the sample presented prediabetes(6); likewise, Chile reports a prevalence of 12.3%, reducing this value to 10.2% at the self-report(7).
In the Peruvian context, the General Law for the Protection of People with Diabetes drives the implementation of the National Program for the Prevention and Care of Patients with Diabetes, in order to improve health and their quality of life(8). In 2015, the prevalence reported by PERUDIAB was 7.0% nationally and 8.4% for metropolitan Lima, with a cumulative prevalence of 19.5 cases per thousand people per year(9). Data from the National Institute of Statistics and Information-INEI-202210(10) confirms an increase in the prevalence of DM(9,11,12), reaching 5.1% of the population over 15 years of age, with a greater impact on women, where geographically the Peruvian coast has the highest prevalence. Two new cases are registered for every 100 people per year(12).
This fact affects the quality of life of people(13), due to long-term complications, especially microvascular complications, such as diabetic retinopathy, chronic renal failure, and diabetic foot, identified as serious threats to physical and mental health, generating not only a high economic cost but also suffering for families and society as a whole(14).
Studies on quality of life in patients with DM show diverse results. In Mexico(15,16), quality of life was rated as good, although there were concerns about sexual functioning(15,17). In Paraguay, quality of life was rated as poor(18); another study indicates that patients with type 2 diabetes and renal failure maintained an average quality of life, with a significant impact on the physical dimension(19) and relatively good levels in the dimensions of physical health and psychological health(20).
These findings underscore the complexity of QoL in patients with type 2 diabetes, with the need for an individualized and multifaceted approach to clinical care and management. However, there is a paucity of data in certain regions and contexts, which highlights the relevance of this study, whose objective was to evaluate the level of quality of life of patients with type 2 diabetes mellitus in a public hospital in the province of Barranca, Lima Region.
METHODS
Study design
Study of quantitative approach, observational method, descriptive, and cross-sectional design.
Study area
The study was conducted in a Ministry of Health-MINSA hospital, category II-1, located in the province of Barranca, Lima-Peru region. It has outpatient clinics for general medicine, pediatrics, pneumology, gastroenterology, cardiology, dentistry, otorhinolaryngology, gynecology and obstetrics, psychology and psychiatry, physical therapy, and health strategies.
Population and sample
The population consisted of 242 patients with DM from the health strategy for the prevention and control of noncommunicable diseases. The sample consisted of 144 patients with type 2 diabetes, determined by means of a finite population formula for descriptive studies, with a 95% confidence interval, a probability of success of 64% and an error of 0.05%. The sampling was simple random, using software called random number generator, with replacement of patients in case of rejection.
Inclusion criteria were considered to be age over 40 years, diagnosis of type 2 DM, with a period of illness of no less than two years, and regular attendance at the clinic for non-communicable diseases, with voluntary participation.
Variables and instrument
Quality of life. It is the evaluation of the objective functioning (capabilities, behaviors) and subjective (satisfaction / dissatisfaction) that the person makes about himself(21,22). It integrates the following dimensions: physical, psychological, social relations, and environment(20).
Gender, identified as female and male, according to the biological perception expressed by the participant and the chronological age reported, were also considered as study variables.
The instrument used to assess quality of life was the "World Health Organization Quality of Life (WHOQOL-BREF)", internationally recognized to determine the profile of quality of life perceived by people and applied in different countries, languages, and cultures(23). The reliability of the instrument was found to be 0.88 in the Peruvian population(24).
The WHOQOL-BREF is applied to the chronically ill, caregivers, people undergoing stressful situations, children, among other groups(25). Quality of life is rated as low, medium, or high, with the higher score representing a better quality of life. In the study, the results were evaluated according to the established algorithm(25).
Procedure
The process was carried out with prior authorization from the hospital and coordination with the health strategy for the prevention and control of non-communicable diseases, first accessing the personal data of each patient according to the registry.
The data were collected between April-June 2021, with the necessary provisions and instruments in view of the health situation in the country(27,28). Patients were contacted by telephone; each patient was identified and invited to participate in the study, receiving information on the objective, procedures, and concerns. They were also informed of the complete information contained in the informed consent form.
Once all the preliminary information was clear, we proceeded with the application of the questionnaire (via telephone), taking approximately 20-25 minutes.
There were some exceptions to the telephone interview, with those patients for whom it was not possible to establish fluid communication for the completion of the questionnaire. For these patients, a home visit was made (total of 14 patients).
Data analysis
For the statistical analysis, the data were previously entered into an Excel database using codes to preserve the anonymity of the participants. Then, the data were transported to Statistica Package for Social Sciences-SPSS v24, using descriptive statistics such as measures of central tendency, frequencies, percentages, and cross-frequency table.
Ethical aspects
The project was submitted to evaluation by the institutional ethics committee, respecting the principles of the World Medical Association. Informed consent was given to each participant.
RESULTS
With respect to the characterization of the sample, Table 1 shows that 70% were aged between 40-64 years; 69% identified themselves as women; 38% were cohabiting and 34% were married; 24% had technical studies and 20% were illiterate.
| Variable | Category | Frequency | Percentage |
|---|---|---|---|
| Sex | Female | 99 | 68.6% |
| Male | 45 | 31.3% | |
| Age | 40 – 64 | 102 | 70.9% |
| 65 – 80 | 42 | 29.3% | |
| Schooling | Iletrado | 29 | 20.1% |
| Primary | 22 | 15.3% | |
| Secondary | 31 | 21.5% | |
| Technical | 35 | 24.3% | |
| University | 27 | 18.8% | |
| Marital status | Single | 11 | 7.64% |
| Cohabitant | 55 | 38.2% | |
| Married | 49 | 34.0% | |
| Divorced/Widowed | 29 | 20.1% |
Figure 1 shows the results of the quality of life, with 86% (124 patients) being rated as medium level QoL.
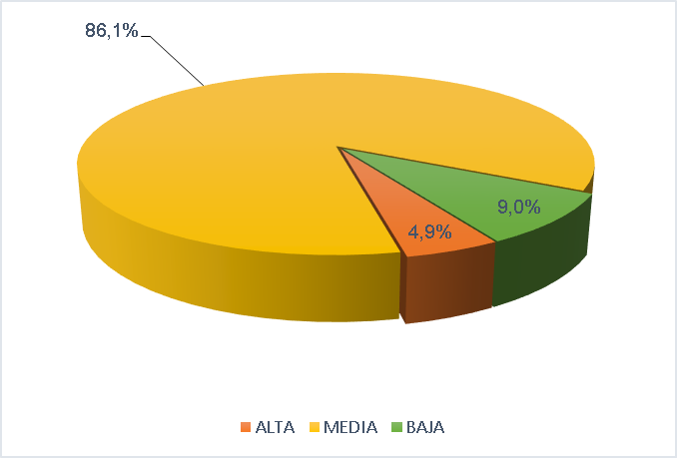
Figure 1: Quality of life of patients with type 2 diabetes, MINSA Hospital, Barranca province, April-June 2021.
In Figure 2, in the social dimension 74% (107 patients) achieved a high level VC, in the psychological and environmental dimension, the VC was medium level (107 and 104 patients respectively), in the physical dimension, 64% (92 patients) achieved a low level VC.
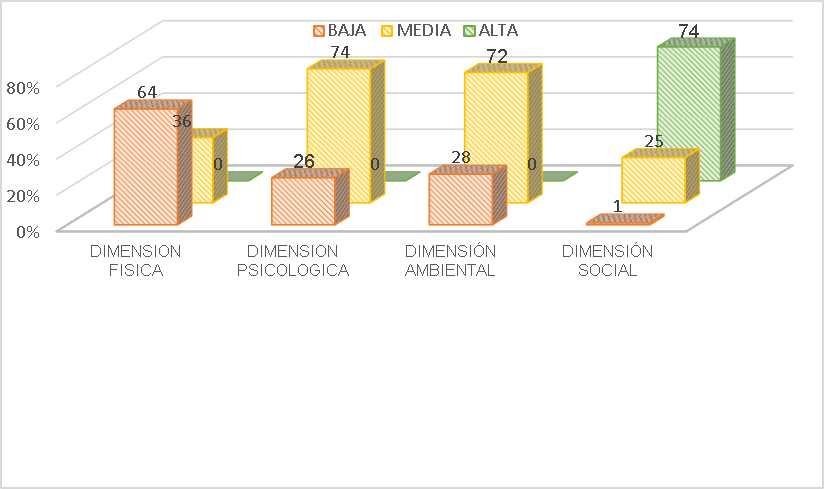
Figure 2: Quality of life of patients with type 2 diabetes by dimensions, MINSA Hospital, Barranca province, April-June 2021.
In Figure 3, medium-level QOL predominated in both sexes (90% and 86% in men and women, respectively), with women perceiving low-level QOL in a higher proportion than men.
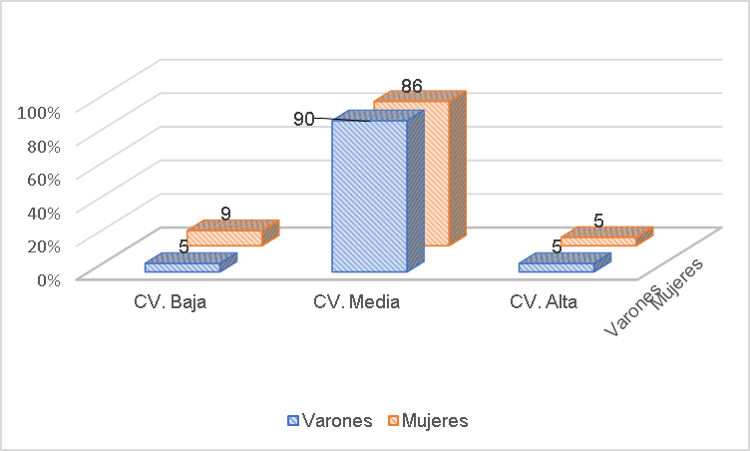
Figure 3: Quality of life of patients with type 2 diabetes according to sex, MINSA Hospital, Barranca province, April-June 2021.
In Figure 4, patients in the 65-80 years age range presented a low level of QOL (29%), while 94% of the 40-65 years age range perceived a medium level of QOL.
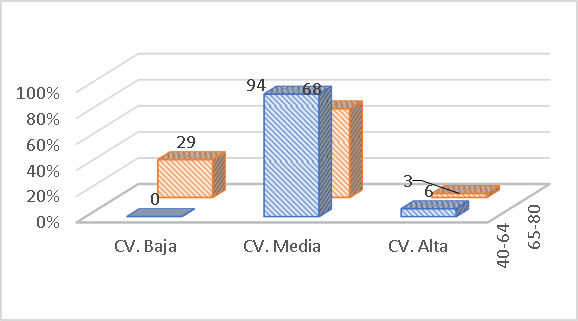
Figure 4: Quality of life of patients with type 2 diabetes mellitus according to age group, Laura Esther Rodríguez Dulanto Hospital, Barranca, April-June 2021.
DISCUSSION
QoL, as a subjective variable, provides a comprehensive perspective of the impact of diseases on people's lives. In the case of type 2 DM, a significant influence on biopsychosocial aspects is observed(25). This statement is based on the difficulty patients face in maintaining a healthy diet, the lack of frequent physical activity, and the prevalence of overweight in this group(25).
The World Health Organization (WHO) supports this concern, given the alarming increase of patients diagnosed with type 2 DM worldwide. In 2014 there were 422 million cases, and by 2019, type 2 DM was positioned as the ninth leading cause of death, with 1.5 million deaths attributed to this disease(30). Figures that underline the urgency that represents in public health for type 2 DM, not only in terms of mortality, but also in terms of its negative impact on the health and QoL of those affected(25). As shown by several studies(15-20).
Certainly, QoL is a term with multiple definitions, since each construction is influenced by the social and cultural environment; a context that conditions the behavior of people, where objective and subjective factors are combined and that will have an impact on one's own life. When old age arrives, changes in lifestyle inevitably occur, which in turn alter the QoL, in addition to the presence of a disease and the complications it brings with it(21).
The findings of the study highlight the need for effective interventions at a global level for people with diabetes, addressing both the medical and socioeconomic aspects associated with this disease(31). The study highlights the public health context experienced in the country during the COVID-19 pandemic, when attention to non-communicable diseases in health services was reduced or suspended as a control measure. This may have aggravated the situation of patients.
When analyzing QoL with the variables sex and age group, the results reveal that both men and women, as well as in the different age groups, QoL was of medium level (Figure 3, 4), although this could vary when considering the time of the disease and the capacity for self-care. This perspective shows the importance of promoting self-care as a key strategy to improve health and prevent chronic diseases, which could raise the level of QoL, both at the individual and community level(17,20).
In terms of QoL dimensions, there is greater affectation in the physical dimension, followed by the psychological, environmental, and social dimensions (Figure 2). Reflecting the complexity of the experience of living with type 2 DM, which not only involves physical, but also emotional, social, and environmental challenges. There is an urgent need for a multidisciplinary and intersectoral approach in the therapeutic approach, which goes beyond glycemic control and integrates psychosocial support, promotion of healthy lifestyles, and improved access to medical care(32).
The study highlights the social relationships, the environment, and the health care received during the COVID-19 pandemic. Varillas(19) reported patient dissatisfaction in sexual life, as a consequence, of the antidiabetic treatment; despite the fact that most of them presented a high level QoL; living with a partner, seems to positively influence QoL, although this does not translate into sexual satisfaction(33).
In the environment-environment, most patients reported living in satisfactory conditions and having economic resources to cover their basic needs, as did the findings of Guzmán et al.(17). However, the lack of opportunities for leisure activities reveals a limitation in QoL. The analysis by dimensions of QoL offers valuable information to health personnel, where it is important to include the family, and thus involve them in the process of patient care and treatment(34). Law Nº28553(8), designed to protect people with diabetes and improve their QoL, still seems to be deficient in the Peruvian health system.
The analysis of QoL by age group revealed (Figure 4) a greater deterioration in people over 65 years of age, possibly attributed to the wear and tear and complications associated with diabetes over the years, as well as to the presence of multiple chronic degenerative diseases(15).
The multidisciplinary and intersectoral approach to DM should prioritize the first level of care, where primary care professionals play a fundamental role, strengthening prevention and health promotion interventions in families and at-risk groups. Comprehensive and preventive care contributes significantly to the QoL and well-being of patients, thus helping to control the disease, delay complications and reduce the impact on public health(35).
To achieve this purpose, it is necessary to expand multiprofessional teams at the primary care level in order to comply with primary care policies. There is a high deficit of personnel and infrastructure at this level of care, given the demographic and epidemiological changes that have been occurring in middle and low-income countries, such as Peru. It is necessary, the confluence of policies and greater investment in health at this level, in order to control and reduce non-communicable diseases, which are the cause of premature deaths in the population.
The scarcity of updated information highlights the importance of continuing to explore QoL in patients with diabetes and to apply more effective interventions considering its associated factors, such as home accompaniment, glucose monitoring, and self-care practices, including healthy diet, use of hemoglucotest, care and prevention of diabetic foot, participation in recreational activities, in addition to strict medical check-ups every 90 days. Need for an increase in the health budget at the central level.
Among the limitations recognized in the study is memory and attention bias, particularly due to the nature of the telephone interviews. The lack of face-to-face interaction and the limited time of the calls may have influenced the quality of responses and the accuracy of the information collected.
In conclusion, the importance of identifying areas of intervention and the need for public health policies and programs that respond to the specific needs of this vulnerable population is highlighted. Despite the limitations, the study findings may guide future research and clinical practice in the field of type 2 DM.
Conflict of Interest Statement: The authors declare no conflict of interest. Work
extracted from the thesis titled "Quality of life in patients with type 2 diabetes at
Hospital de Supe." Universidad Nacional de Barranca. https://repositorio.unab.edu.pe/item/d938ca72-44a3-44b4-bf8c-f7bb81449b8a
Author Contributions: NSCM, MARC, and KOV contributed to the conception of the
article, data collection, analysis and interpretation, drafting, and approval of the final
version. Additionally, MEM and ESSC contributed to drafting, critical revision, and approval
of the final version.
Funding: Self-funded.
Received: May 7, 2024
Approved: June 30, 2024
Corresponding Author: Kattia Ochoa-Vigo
Address: Calle Jonh Neper 104, Apt. 303, Urb. San Borja Sur, Lima 41, Peru.
Phone: (+51) 995920067
Email: kochoa@unab.edu.pe
Article published by the Journal of the faculty of Human Medicine of the Ricardo Palma University. It is an open access article, distributed under the terms of the Creatvie Commons license: Creative Commons Attribution 4.0 International, CC BY 4.0 (https://creativecommons.org/licenses/by/4.0/), that allows non-commercial use, distribution and reproduction in any medium, provided that the original work is duly cited. For commercial use, please contact revista.medicina@urp.edu.pe.
BIBLIOGRAPHIC REFERENCES
