ARTICULO ORIGINAL
REVISTA DE LA FACULTAD DE MEDICINA HUMANA 2019 - Universidad Ricardo PalmaDOI 10.25176/RFMH.v19i4.2194
EVALUATION OF THE PREVALENCE OF INFECTION BY ATYPICAL GERMS IN PATIENTS WITH COMMUNITY-ACQUIRED PNEUMONIA IN A PERUVIAN REFERENCE HOSPITAL
EVALUACIÓN DE LA PREVALENCIA DE INFECCIÓN POR GÉRMENES ATÍPICOS EN PACIENTES CON NEUMONÍA ADQUIRIDA EN LA COMUNIDAD EN UN HOSPITAL DE REFERENCIA PERUANO
Alonso Soto1,2,a
1 Instituto de Investigación en Ciencias Biomédicas. Facultad de Medicina. Universidad Ricardo Palma.
2 Departamento de Medicina. Hospital Nacional Hipólito Unanue
a Médico Internista. PhD in Health Sciences
ABSTRACT
Objective: To determine the prevalence of infection due to atypical microorganisms in cases of community-acquired pneumonia in adult inmunocompetent patients seeking attention in the Hospital Nacional Hipolito Unanue. Material and Methods: Adult inmunocompetent patients seeking medical attention in the emergency ward of Hospital Hipolito Unanue with diagnosis of community-acquired pneumonia were evaluated between september 2008 and january 2009. Blood samples were drawn for Mycoplasma pneumoniae and Chlamydia pneumoniae serology, by the detection of M Inmunoglobulin by ELISA technique.Results: We recruited 85 patients. The average age was 65.33 ± 21.43 years. We found 3 cases with positive IgM serology against M. pneumoniae and 1 case positive against C. pneumoniae. The antibody titers against M. pneumoniae had a highly significant correlation with the age (r=-0,28; p<0,01). We also found a statistically significant difference between the titers of antibodies against M. pneumoniae and those correspondent to C. pneumoniae (r=0.29; p<0,01). Conclusion:Infection due to atypical microorganisms doesn’t seem to be a frequent condition in inpatients with diagnosis of Community-acquired pneumonia. Research in larger populations, including outpatients should be done, in order to define the role of atypical pathogens in cases of Pneumonia at a national level.
Key words: Pneumonia, Mycoplasma pneumoniae , Chlamydia pneumoniae
RESUMEN
Objetivo: Determinar la prevalencia de infección por gérmenes atípicos evaluada mediante la determinación de anticuerpos IgM en casos de neumonía adquirida en la comunidad en pacientes adultos inmunocompetentes atendidos en el Hospital Nacional Hipólito Unanue. Material y Métodos: Se evaluaron a aquellos pacientes adultos inmunocompetentes que acudieron a la emergencia del Hospital Hipólito Unanue con neumonía adquirida en la comunidad entre setiembre del 2008 y enero del 2009. Se tomaron muestras de sangre para realizar serología para Mycoplasma pneumoniae y Chlamydia pneumoniae mediante la detección de niveles de inmunoglobulina M determinados por prueba de ELISA. Se evaluaron a aquellos pacientes adultos inmunocompetentes que acudieron a la emergencia del Hospital Hipólito Unanue con neumonía adquirida en la comunidad entre setiembre del 2008 y enero del 2009. Se tomaron muestras de sangre para realizar serología para Mycoplasma pneumoniae y Chlamydia pneumoniae mediante la detección de niveles de inmunoglobulina M determinados por prueba de ELISA. Resultados: Se reclutaron 85 pacientes. La edad promedio fue de 65.33 ± 21.43 años. Se encontraron 3 casos de pacientes con serología positiva a IgM frente a M. pneumoniae y 1 caso positivo a C. pneumoniae. Los títulos de anticuerpos contra M. pneumoniae tuvieron una correlación altamente significativa con la edad (r=-0,28; p<0,01). se encontró una correlación estadísticamente significativa entre los índices de anticuerpos IgM frente a M. pneumoniae y C. pneumoniae (r=0.29; p<0,01). Conclusión: La infección por gérmenes atípicos no parece ser una condición frecuente en pacientes hospitalizados con diagnóstico de Neumonía adquirida en la Comunidad. Se deben realizar estudios en poblaciones mayores utilizando serología pareada o estudios moleculares, incluyendo pacientes ambulatorios a fin de definir el rol de patógenos atípicos en casos de Neumonía a nivel nacional.
Palabras Clave: Neumonía, Mycoplasma pneumoniae , Chlamydia pneumoniae
Community-acquired Pneumonia (CAP) is still an important cause of mortality and morbidity worldwide1. In Peru, lower respiratory tract infections have represented the first cause of mortality over the past three decades.
CAP’S etiology is of paramount importance when taking decisions regarding the most appropriate therapeutics. Without local studies, empirical therapy for pneumonia turns out to be usually an extrapolation of established recommendations on guides developed on milieus distinct to Peruvian’s, having maybe a typical bacteriology distinct to Peruvian’s. Thus, there is an urgent need to count on national studies in order to explain CAP bacteriology of cases treated at hospitals.
According to numerous studies worldwide, and to Latin American and Peruvian context, the most common cause of CAP is Streptococcus pneumoniae.2,3infection. Many series mention Mycoplasma pneumoniae as another prevalent organism that even surpass pneumococcus on severe pneumonia4 Other related bacteria include Haemophilus influenzae , Moraxella catharralis and Enterobacteriacea5.
One of the most discussed aspects of Community-Acquired Pneumonia diagnosis is initial empirical therapy (when microbiological studies’ results are not on hand), which must be based on bacteriology from the community where the patient belong. Amoxicillin represents initial empirical therapy to community-acquired pneumonia for outpatient treatment, according to recommendations by British Thoracic Society6 ,, National Institute for Health and Care Excellence7 , and at Peruvian level, recommendations by Sociedad Peruana de Enfermedades Infecciosas y Tropicales8. While it is true that amoxicillin can be used as monotherapy, this antibiotic have no effect against atypical such as macrolide and doxycycline9 . Nevertheless, since local studies on atypical germs prevalence, usefulness of adding drugs having effect against this pathogens will continue to be a question from the therapeutic point of view.
Regarding pneumonia with hospital treatment, a wider coverage is indicated. Benefit in adding treatment for mycoplasma and chlamydia is not determined. However, coverage against atypical is often added due to possibility of legionella, a pathogen associated to severe pneumonia6,7,9.
On the foregoing, it is essential to carry out studies based on national casuistry so they may allow to establish rational therapeutic algorithms. In Peru, unfortunately, there are no enough studies among adults in order to draw conclusions, though a study of children suggest a frequency of up to 30% regarding atypical germs10.
The objective of our study was to determine the prevalence of infection by atypical germs in community-acquired pneumonia cases in immunocompetent patients attended at Hipólito Unanue National Hospital from March 2008 until January 2009.
METHODOLOGY
Type of study, population and sample
It was carried out a descriptive and cross – sectional study. The universe of patients embraced those patients who went to emergency and hospital services at Hipólito Unanue Hospital from March 2008 until January 2009.
On the basis of a proportion of atypical prevalence of 10% (with a 95% confidence interval from 0.05 to 0.15), the sample calculated based on the application of the formula of proportions confidence interval [CI= p +/- z √ (p) (q)/n] embraced 75 patients (where CI=0.05-0.15, z=1.96 p=0.1 q=0.9).
Sampling and patient recruitment
There was a successive recruitment embracing patients that go to Hipólito Unanue National Hospital, from emergency, hospitalization and outpatient department of medicine and pulmonology, who met inclusion criteria and agreed to successively provide their informed consent until meeting the specified sample size.
Inclusion and exclusion criteria
It included patients with community-acquired pneumonia clinical diagnosis, on the basis of these criteria: time of sickness no longer than ten days; two of next symptoms: fever, cough with sputum, respiratory distress or pleuritic chest pain; abnormal findings on physical examination (crackling rales, bronchophony or pectoriloquy) or chest x-ray showing abnormal findings compatible with pneumonia: spotted alveolar infiltrate or diffuse interstitial pattern; and agreement of participating in the study. It excluded patients under 18, patients with tuberculosis or AIDS, pregnancy, chest x-ray with presence of suggestive infiltrate of tuberculosis (milia, cavities in the lungs or spotted apical).
Procedures
After obtaining informed consent, a form was filled, which contained important epidemiological and clinical data. Blood samples were taken in order to carry out serology on Mycoplasma pneumoniae and Chlamydia pneumoniae via detection of immunoglobulin M levels, on the basis of ELISA test. Patients were called to carry out convalescent serum serology, two weeks after sample collection of acute infection. Patients were reassessed 72 hours after starting empirical antibiotic therapy, at discharge in inpatients and after 14 days.
Statistical Analysis
Numeric variables are presented as mean ± standard deviation (or medians and interquartile ranges on abnormal distributions) or as frequencies and percentages for those in the nominal scale. For bivariate analysis, qualitative variables will be analyzed through Chi – square test (x2) and quantitative variables through Student’s t or through Wilcoxon-Mann-Whitney test in case of abnormal distribution. In addition, a secondary analysis measuring association of proposed variables with serology for atypical. Differences between variables were considered significant with a p<0.05value. Data were analyzed using the statistical package STATA v11.
Ethical aspects
Informed consent of all respondents was accomplished. A written informed consent was employed in order to fully document voluntary participation of patients. In case of illiterate patients, it was attached a relative’s signature who witness having provided pertinent information.
RESULTS
85 patients were recruited. Average age was 65.33 years, with a standard deviation of 21.43 years. It was found a higher proportion (without statistical significance) of male sex: 55.1 vs 44.9%. The highest percentage of patients were from El Agustino district (figure 1).

Figure 1: Distribution of patients according to place of origin
Table 1. Population Characteristics
| Variable | Value |
| Age | 65.36 +/- 21.43 |
| Male sex | 35 (41.11%) |
| Temperature (average and CIR) | 37.6 (0.4) |
| Abnormal finding on Physical Examination | 63 (74.12%) |
| White blood cell count (average and CIR) | 12000 (5890) |
| Abnormal Chest X-ray | 74 (87.06%) |
| Deceased patients | 10 (11.76%) |
Result of Serology for atypical germs
Mycoplasma pneumoniae
2 positive results were found on initial serology for M.pneumoniae, while a case of positive results (with a baseline sample negative) was found among 8 patients to those who underwent a convalescent serology after two weeks of obtaining the first sample. A serology for IgG antibody detection was carried out in a random subsample of patients. Among 25 included patients, we found 18 (72%) positive, 1 (4%) indeterminate and 6 (24%) negative results.
Chlamydia pneumoniae
A positive result and an indeterminate result were found on initial serology. On serology control carried out on 8 patients who were initially negative, any positive result was found. A secondary analysis correlating serology with studied variables. Antibody titers against M.pneumoniae got a highly significant correlation with age (r=-0.28; p<0.01) (Figure 2).

Figure 2: Antibody titers concerning M. pneumoniae and age
Finally, a statistically significant correlation was found between levels of antibodies against M. pneumoniae y C. pneumoniae Finalmente, se encontró una correlación estadísticamente significativa entre los índices de anticuerpos frente a M. pneumoniae y C. pneumoniae (r=0.29; p<0.01) (Figure 3).
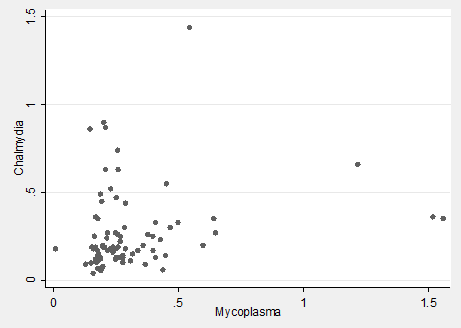
Figure 3: Correlation between levels of antibodies against M. pneumoniae y C. pneumoniae
Table 2. Multiple linear regression model for correlating antibody titers against M.pneumoniae y C.pneumoniae.
| Beta coefficient (CI95%) p-value | p-value | |
| Antibodies vs.M.pneumoniae | 0.31 (0.04; 0.58) | 0.03 |
| Age | 0.002 (-0.001;0.005) | 0.13 |
| Sex | 0.07 (-0.03;0.16) | 0.19 |
Pneumonia represents one of the main initial diagnosis in inpatients. In our experience, coverage against atypical germs in terms of using new macrolide results very frequent in Metropolitan Lima most hospitals’ emergency and hospital services. However, this medicine have a high cost and this may be a barrier in order to complete treatment. In our milieu, there are no studies that document the existence of infection by atypical in adult patients with community-acquired pneumonia. Management guidelines from American Thoracic Society (ATS) and Infectious Diseases Society of America (IDSA)9 yand Latin American Thoracic Association11 (ALAT, for its acronym in Spanish) suggest coverage against atypical with a strong degree of recommendation, while those guidelines from BTS6 and NICE7,as well as Peruvian guideline from SPEIT8 continue recommending beta lactams as first-line agent, without necessarily including coverage against atypical.
Our preliminary results show an atypical germs low prevalence in community-acquired pneumonia from August until December in inpatients at Hipólito Unanue Hospital. This finding does not necessarily mean to discard atypical germs as pneumonia causes. In particular, it is known the seasonal, and even annual, fluctuation of prevalence of infection by Mycoplasma pneumoniae.12 As additional significant findings, a negative association between age and levels of antibodies against M. pneumonia was found. This agrees with most reports that state the highest prevalence of mycoplasma pneumonia in young age groups. Regarding our population is largely composed of elderly, M. pneumonia infection low prevalence is understandable. Nevertheless, this could be due to lower immune response in elderly. Our study did not evidence any correlation between serology for Mycoplasma pneumoniae or Chlamydia pneumoniae with any of parameters evaluated on physical examination, type of infiltrate on chest x-ray or patient survival. On this matter, it is important to highlight that many studies have demonstrated lack of association in terms of clinical or radiologic abnormalities related to atypical germs infection; thus, the term “atypical pneumonia”, first coined for identifying prominent symptoms in upper respiratory tract and interstitial infiltrate in chest x-ray, has been left behind, preferring the term “atypical germs pneumonia”.
A statistically significant correlation between M. pneumoniae y C. pneumonia regardless of patient’s age and sex was found. This could be due to induction of nonspecific immunologic responses that provoke a general response of production of antibody production with cross-reactivity
One limitation in our study was low proportion of patients who underwent a serology control, mainly due to loss during the follow-up and deceases. Even though we could not achieve the programmed serology, we consider our study represents a contribution to Peruvian epidemiology, because it is one of the few national studies focused on search for atypical germs in community-acquired pneumonia diagnosis inpatients.
Another interesting aspect is that a subgroup of patients were able to undergo an IgG serology for M. pneumonia, finding a high prevalence of suggestive titers of previous exposure of germs. That is to say, despite of frequent exposure in population, pneumonia patients who require hospitalization would show a low prevalence of Mycoplasma pneumoniae infection. Among atypical germs, besides Mycoplasma pneumoniae and Chlamyidia pneumoniae, we have Legionella pneumophila, mainly related to cases with a greater severity8,13. However, there are still not indigenous cases described in Peru.
Though lack of country-level studies’ evidence, and possibly in large part due to increasing pressure of pharmaceutical industry, community-acquired pneumonia treatment is often based on using extended-spectrum-against-pneumococcus fluoroquinolones (misnamed “respiratory” fluoroquinolones), although their use in common lower respiratory tract infections should be exceptional14. Furthermore, many doctors consider obsolete or ineffective the use of drugs like amoxicillin or doxycycline. Taking into account the huge costs in terms of money and development of bacterial resistance at which these decisions may lead, it is imperative to define the election of effective and affordable chemotherapeutic agents for our population. Our findings reinforce the need to carry out multicenter national studies on a larger scale, in both outpatients and inpatients, in order to define the need of employing antimicrobial agents with coverage against atypical germs. On the other hand, it is evident the need to carry out clinical trials that compare antibiotic therapy schemes with and without coverage against atypical germs, due to inconclusive evidence regarding usefulness in adding antibiotic coverage against these pathogens15.
In conclusion, our study suggests a relatively low prevalence of atypical germs infection in community-acquired pneumonia inpatients. Studies on a larger scale should be carried out, in order to measure actual prevalence of atypical germs infection including seasonal variations, as well as clinical trials that compare use of beta lactams with association of beta lactams and macrolide.
Acknowledgements
To Doctor Vilma Acurio, for her help in sample processing. To Doctors Manuel Montellanos and Marita Astocondor, for their cooperation on patient recruitment.
Authorship credit: The autor took part in the origin of the idea, project desing, data collection and interpretation, analysis of results and preparation of the manuscript of this research work.
Funding: The study was funded by Ricardo Palma University.
Conflict of interest: The autor states not to have any conflict of interest.
Received: March 20th, 2019
Approved: August 29th, 2019
Corresponde: Alonso Soto
Address: Cesar Vallejo 1390, El Agustino 15007
Phone number: (01) 3625700
Email: sotosolari@gmail.com
Bibliographic References
