Introducción
Coffee is the most consumed psychoactive agent worldwide. It has a pH of 5.0
1
and is composed of biologically active elements such as caffeine, diterpenes, and chlorogenic acids
2
. In the gastrointestinal tract, coffee has beneficial effects with organoleptic and physiological properties
3
. It stimulates the production of intestinal sounds, gas, and produces an intraluminal effect in the digestive tract
4
.
Surgery involves mechanical and biological stress on the body
5
. In the lower digestive tract, neurogenic mechanisms that occur during surgery inhibit sympathetic stimulation and increase adrenergic motor neuron activity
6
. Additionally, the inflammatory process promotes the release of nitric oxide and prostaglandins, which subsequently inhibit smooth muscle contractility
7
8
. Moreover, anesthetic agents used during surgery prolong gastric emptying time, increasing the risk of postoperative nausea and vomiting
9
10
. Altogether, these factors contribute to the development of paralytic ileus, extending the patient’s recovery time
11
12
.
Many studies show the effects of caffeinated coffee and its biological action in inducing pressure waves and prokinetic activity in the digestive tract
13
. The mechanism through which motor stimulation of intestinal transit occurs is neurohumoral, blocking adenosine A1 and A2 receptors
14
. Brown SR et al. have established that coffee induces propulsive motor activity for approximately 90 minutes, similar to stimulation after food intake, suggesting it as an agent of choice in initiating oral intake in gastrointestinal surgical patients
15
16
. The objective of this study is to present the clinical effects of initiating oral intake with coffee in patients undergoing lower gastrointestinal surgery.
Materials and Methods
A descriptive study was conducted on patients scheduled for elective lower gastrointestinal tract surgery. Patients over 18 years old, of both sexes, with benign pathology, who signed informed consent prior to the procedure, were included. Patients who developed complications during surgery were excluded.
Variables considered for descriptive analysis included history and characteristics of the surgical procedure, surgical time, intraoperative bleeding, and type of procedure performed.
The coffee preparation was based on the dilution proposed by Satish et al. (890 ml of deionized water heated to 85 °C with 28.35 grams of coffee). Postoperative patients consumed the beverage three times daily, receiving 100-150 ml per intake at 7:00, 12:00, and 17:00. The final product was offered to the patient at an intake temperature of 45.0 °C.
Similarly, in the study by Hasler-Gehrer S et al., three sequential doses were given, as also presented in the meta-analysis by Cornwall HL et al. Each patient was informed that each prepared beverage intake would be 50 mL, with clinical effects of initiating oral intake with coffee subsequently assessed.
Patients were evaluated daily during their postoperative period until hospital discharge. Categorical variables used to determine the effects of coffee implementation in early enteral nutrition included the first bowel movement, gas passage, time of solid tolerance, hospital stay, first bowel movement, and postoperative complications (postoperative ileus).
The study was approved by the Ethics Committee of the participating unit: Hospital de Especialidades de Puebla, Centro Médico Nacional Gral. de Div. Manuel Avila Camacho. Personal data was handled with strict confidentiality and exclusively for scientific purposes.
Results
A sample of 14 patients was included: 9 women (64.3%) and 5 men (35.7%). The mean age at intervention was 51.7 years (SD ± 7.5); the average surgical intervention time was 257.3 minutes (SD ± 32.6) with an average blood loss of 250 milliliters (SD ± 45.6).
The average solid tolerance time was 24 hours (SD ± 2.4) in women and 12 hours (SD ± 1.8) in men, with a mean of 18 hours across all patients undergoing lower gastrointestinal surgery.
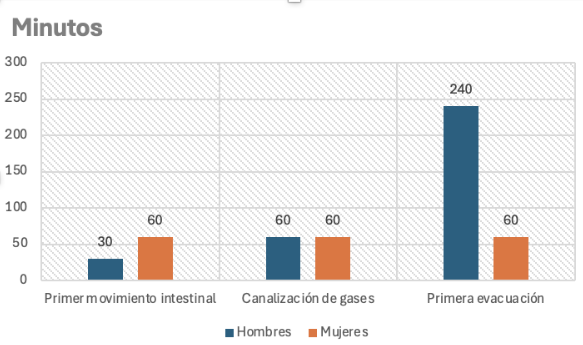
The average hospital stay was 2.5 days (SD ± 0.9). The time interval between surgery and the first bowel movement was 4.5 hours after coffee infusion (SD ± 0.75), with a mean difference between men and women of 60 minutes (SD ± 23.5) versus 240 minutes (SD ± 75.6) respectively. The incidence of postoperative paralytic ileus following gastrointestinal surgery was present in 8.3% of the sample. Patients reported no adverse effects following coffee infusion.
The clinical effects of coffee infusion in relation to time of occurrence are shown in Figure 1.
Discussion
Multiple studies have proposed coffee as the prokinetic of choice for gastrointestinal tract surgical procedures. The benefit of coffee corresponds to the induction of propulsive motor activity in the digestive tract. Previously, coffee consumption was thought to produce adverse effects and complications during the postoperative period; however, recent studies have demonstrated its usefulness in early progression of oral intake and its safety for routine implementation
17
18
19
.
A systematic review of 601 patients by Eamudomkarn et al. in patients undergoing elective lower gastrointestinal tract surgery, who received coffee infusion three times a day post-surgery, showed a reduction in time to first bowel movement to nine hours, gas passage time to seven hours, first bowel movement to four hours, and solid tolerance in 0.74 days
20
. In our study, the mean time after coffee infusion for the first bowel movement was 4 (SD ± 3) hours, gas passage 1 (SD ± 1.5) hour, first bowel movement 1 (SD ± 2.3) hour, and solid tolerance between 18 (SD ± 12) hours.
The main limitation of this study was the small sample size, as patient participation was low due to lack of willingness to enter the study or low adherence to instructions. Further clinical studies are required to reach adequate conclusions and to extrapolate findings to other types of gastrointestinal surgeries.
Conclusions
Initiating oral intake with coffee infusion in patients undergoing lower gastrointestinal surgery promotes motor activity, reduces time to onset of bowel sounds, gas passage, and effective bowel movements. A decrease in the incidence of postoperative paralytic ileus was demonstrated following coffee infusion administration. Coffee infusion implementation benefits early progression to a soft diet.